The Future of Knee Osteoarthritis Treatment: Best Practice, Innovation, and State of the Art
One third of adults between the ages of 18 and 64 have arthritis,1 and the lifetime risk of developing knee osteoarthritis (OA) by the age of eight-five is 45%.2 The prevalence of knee OA is very high, and it’s continuing to rise.
OA happens when cartilage, the smooth covering on the ends of our bones, starts to break down. This loss in cartilage can cause bone-on-bone contact during movement as well as undesirable bone growth, called bone spurs. These degenerative changes cause swelling, pain and stiffness, all of which contribute to a reduced quality of life, and need to be addressed by a knee osteoarthritis treatment plan.
There are many national and international organizations, including Osteoarthritis Research Society International (OARSI), National Institute for Health and Care Excellences (NICE), European League Against Rheumatism (EULAR) and the American Academy of Orthopaedic Surgeons (AAOS), that develop clinical guidelines describing best practices for patient care. These guidelines are based on scientific evidence and recommendations by experts in the area.
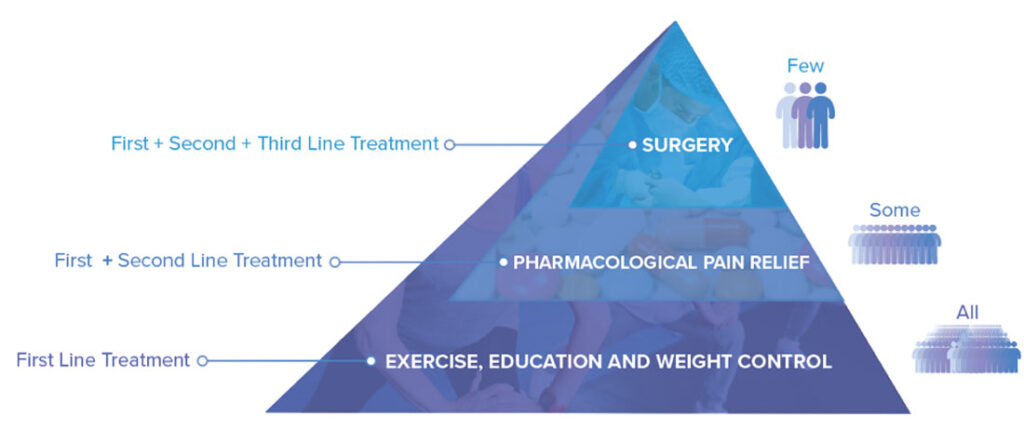
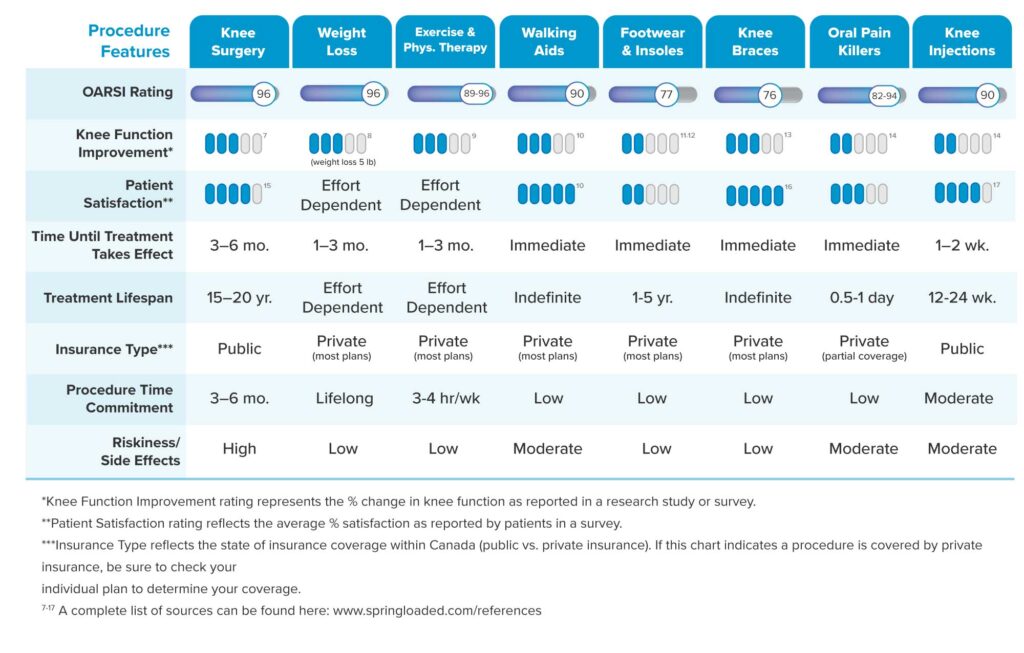
Currently, standard treatment options for knee OA are based on the severity of the disease. Exercise, education and weight management are recommended as a first line of treatment for all patients with knee OA.3 There is strong evidence around exercise to reduce pain and maintain muscle strength.4 Weight management is also important because the load on the knee joint during activity is 2-7X higher than the actual amount of body weight applied.5 So, even a small reduction in body weight can greatly reduce the loading experienced in the joint.

For people who do not find relief from first line treatments, the recommended second line of treatment (in combination with first line treatments) is pharmacological pain relief.3 There are many medications that can be used to manage knee OA symptoms including oral, topical and injections. However, the long-term use of pain medications is associated with undesirable side effects and can cause health concerns.6 For people who have exhausted first and second line treatments, surgery is a treatment option for severe knee OA cases.3 Surgery can be effective for some patients, however, it is very invasive and costly, and over 50% of patients still experience pain after surgery.7 This could be due to many factors, including whether or not surgery was an appropriate intervention in the first place.
These treatment options are based on strong evidence and are the standard of care for knee OA patients today. However, there is exciting research happening on new and promising treatment options, including disease modifying drugs for OA, regenerative medicine approaches, and joint offloading techniques.
Disease Modifying OA Drugs
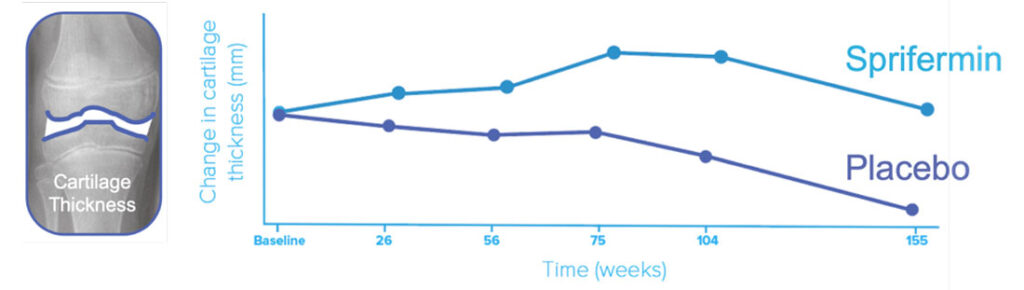
Traditional drugs recommended for knee OA are effective for addressing pain, but they do not delay disease progression or reverse joint damage. As well, because they are frequently associated with adverse side effects when used in the long-term,6 pharmacological researchers have started developing drugs that are intended to promote cartilage repair, prevent undesirable bone growth, reduce pain and minimize potential side effects. This class of drugs is called disease modifying osteoarthritis drugs (DMOADS). One of the more promising disease modifying OA drugs that is now being tested in humans is called “Sprifermin”. This drug is made up of a molecular compound that helps promote the growth of healthy cartilage. A study published last year showed that regular injections of Sprifermin resulted in improved cartilage thickness compared to a placebo, however the effect on clinical outcomes was uncertain.8 While these results are promising, more studies are needed to understand the effect of Sprifermin on patient symptoms, and to verify the long term safety and efficacy of the drug in humans.
Regenerative Medicine Approaches
Regenerative medicine is a field of research that uses the power of the cells found in our own body to heal and regenerate damaged tissues or organs, such as damaged cartilage in knees with OA. One regenerative medicine approach is called stem cell therapy. Stem cells can be harvested from your body, differentiated and grown into the desired cell type, and inserted back into your body. The goal of this therapy for knee OA is to heal and regenerate damaged cartilage in the knee joint. While research continues to advance in this area and shows promise for the future, there are still ongoing challenges in being able to produce cartilage that has the same characteristics as the original cartilage found in our bodies.10 Currently, there is a lack of clinical trial evidence to determine whether these procedures are safe and effective, and as of today, Health Canada has not approved any stem cell therapies for use in humans.11
Joint Offloading Techniques
In contrast to DMOADs and Regenerative Medicine, joint offloading is a well-established core principle of conservative care for knee OA. Cyclical loading and offloading of the joint, for example when walking or climbing stairs, is critical for the maintenance of healthy cartilage. The normal distribution and amount of loading in the knee changes with knee OA, and research has shown that increased loads in the knee joint contribute to the initiation and progression of knee OA.12 Joint offloading aims to reduce and redistribute these loads to avoid further damage and potentially encourage healing within the knee joint.
The knee joint has three compartments where bones meet: the medial tibiofemoral compartment, the lateral tibiofemoral compartment, and the patellofemoral compartment. Knee OA can affect any of these three compartments in the joint.
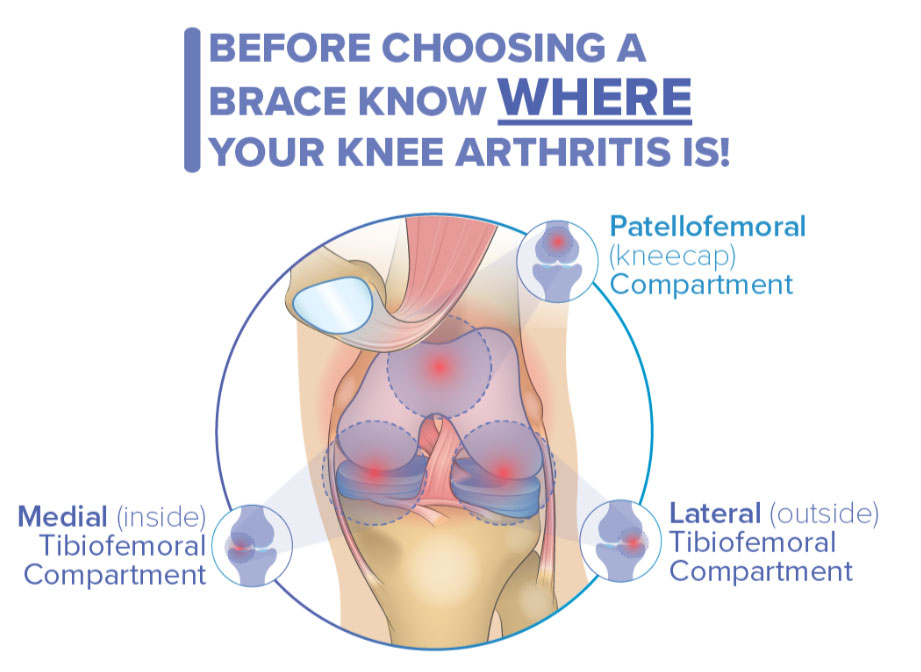
Knee braces for osteoarthritis have been around for decades and there are hundreds of options available. One of the most common types of knee braces are known as “uni-compartment offloaders”. They are designed to offload compressive forces from one side of your knee. They do this by applying a force to the side of your knee to “open up” the joint space on the opposite side and redistribute the forces normally going through the knee across a larger area. Uni-compartment offloader braces are cost-effective and minimally invasive treatments that can reduce pain, improve function, and potentially delay the progression of knee OA for the right patients.13 However, traditional knee braces have one main limitation: they are designed for use in patients with uni-compartmental knee OA affecting one tibiofemoral compartment (ie. one side of the knee). This makes up only 3-20% of all knee OA patients,14, 15 while the majority of patients are likely to have OA in two or all three compartments of their knee.16 This means that traditional knee braces are not optimized for the majority of patients with bi- or tri-compartmental knee OA, which may limit their effectiveness to reduce pain and improve knee function.
Levitation Tri-Compartment Offloader Knee Brace
The benefits and limitations of traditional knee braces, together with the well-established clinical guidelines focused on exercise and weight loss to accomplish joint offloading, formed the motivation for Spring Loaded Technology to develop a new type of brace. The Levitation Tri-Compartment Offloader knee brace was designed to reduce knee pain and improve mobility for patients with patellofemoral or multicompartment knee OA. Levitation’s novel brace uses a powerful silicone liquid spring that provides knee extension assistance to decrease compressive forces in the knee. It is the only brace designed to relieve knee pain and assist mobility by reducing forces in all three compartments of the knee, including the often affected patellofemoral compartment. By simultaneously reducing the loads experienced in both the tibiofemoral and patellofemoral knee joint compartments, Levitation aims to reduce pain, avoid further joint damage and potentially encourage healing within the knee joint. Patients with knee OA who experience pain during activities such as getting up from a seated position, going up or down stairs or walking uphill are likely to benefit from Levitation’s unique technology.

Research conducted thus far on the brace shows that the offloading effect of the brace (when weight bearing) is similar to what would be achieved by losing 45 pounds of body weight.17 An independent study showed that the brace can reduce patellofemoral and tibiofemoral joint contact forces by over 40%.18 In a survey based study of current Levitation brace users, 95% of users reported reduced pain since using the Levitation brace.19 As well, studies with the military have shown that use of Levitation may improve physical performance of military personnel with knee injuries.
Among several other projects, we are now beginning research that will explore the potential benefits of the brace on joint loading and muscle activity using gait analysis and real-time imaging techniques at the University of Calgary. We are also planning a clinical trial to evaluate the efficacy of the brace to reduce pain and improve function in a large group of knee OA patients.
References
- Jafarzadeh, S.R., Felson, D.T., 2018. Updated Estimates Suggest a Much Higher Prevalence of Arthritis in United States Adults Than Previous Ones. Arthritis Rheumatol. 70, 185–192. https://doi.org/10.1002/art.40355
- Murphy, L., Schwartz, T.A., Helmick, C.G., Renner, J.B., Tudor, G., Koch, G., Dragomir, A., Kalsbeek, W.D., Luta, G., Jordan, J.M., 2008. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Care Res. 59, 1207–1213. https://doi.org/10.1002/art.24021
- GLA:D Canada. Treatment for Osteoarthritis.Accessed online from https://gladcanada.ca/index.php/treatment-for-osteoarthritis/ on 19 March 2020.
- Fransen, M., McConnell, S., Harmer, A., Van der Esch, M., Simic, M., KL, B., 2015. Exercise for osteoarthritis of the knee (Review). Cochrane Database Syst. Rev. https://doi.org/10.1136/bjsports-2016-096104
- Messier, S.P., Gutekunst, D.J., Davis, C., DeVita, P., 2005. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum. 52, 2026–2032. https://doi.org/10.1002/art.21139
- Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr Cartil 2008;16:137–62. https://doi.org/10.1016/j.joca.2007.12.013.
- Becker, R., Bonnin, M., Hofmann, S., 2011. The painful knee after total knee arthroplasty. Knee Surgery, Sport. Traumatol. Arthrosc. 19, 1409–1410. https://doi.org/10.1007/s00167-011-1625-7
- Hochberg, M.C., Guermazi, A., Guehring, H., Aydemir, A., Wax, S., Fleuranceau-Morel, P., Reinstrup Bihlet, A., Byrjalsen, I., Ragnar Andersen, J., Eckstein, F., 2019. Effect of Intra-Articular Sprifermin vs Placebo on Femorotibial Joint Cartilage Thickness in Patients with Osteoarthritis: The FORWARD Randomized Clinical Trial. JAMA – J. Am. Med. Assoc. 322, 1360–1370. https://doi.org/10.1001/jama.2019.14735
- Hochberg, M. et al. OP0059 Efficacy and safety of intra-articular sprifermin in symptomatic radiographic knee osteoarthritis: pre-specified analysis of 3-year data from a 5-year randomised, placebo-controlled, phase ii study. Ann. Rheum. Dis. 77, 80 LP – 81 (2018).
- Escobar Ivirico, J.L., Bhattacharjee, M., Kuyinu, E., Nair, L.S., Laurencin, C.T., 2017. Regenerative Engineering for Knee Osteoarthritis Treatment: Biomaterials and Cell-Based Technologies. Engineering 3, 16–27. https://doi.org/10.1016/J.ENG.2017.01.003
- Government of Canada. (2020) Health Canada Policy Position Paper – Autologous Cell Therapy Products. Accessed online from https://www.canada.ca/en/health-canada/services/drugs-health-products/biologics-radiopharmaceuticals-genetic-therapies/applications-submissions/guidance-documents/cell-therapy-policy.html on 19 March 2020.
- Andriacchi, T.P., Favre, J., Erhart-Hledik, J.C., Chu, C.R., 2015. A Systems View of Risk Factors for Knee Osteoarthritis Reveals Insights into the Pathogenesis of the Disease. Ann. Biomed. Eng. 43, 376–387. https://doi.org/10.1007/s10439-014-1117-2
- Steadman RJ, Briggs KK, Pomeroy SM, Wijdicks CA. Current state of offloading braces for knee osteoarthritis. Knee Surgery, Sport Traumatol Arthrosc 2016;24:42–50. https://doi.org/10.1007/s00167-014-3305-x.
- Heekin, R.D., Fokin, A. a., 2014. Incidence of Bicompartmental Osteoarthritis in Patients Undergoing Total and Unicompartmental Knee Arthroplasty: Is the Time Ripe for a Less Radical Treatment. J. Knee Surg. 27, 77–82. https://doi.org/10.1055/s-0033-1349401
- Shahid, M.K., Al-Obaedi, O., Shah, M., 2018. Prevalence of Compartmental Osteoarthritis of the Knee in an Adult Patient Population: A Retrospective Observational Study. EC Orthop. 10, 774–780.
- Duncan, R.C., Hay, E.M., Saklatvala, J., Croft, P.R., 2006. Prevalence of radiographic osteoarthritis – It all depends on your point of view. Rheumatology 45, 757–760. https://doi.org/10.1093/rheumatology/kei270
- Budarick, A.R., MacKeil, B.E., Fitzgerald, S., Cowper-Smith, C.D., 2020. Design Evaluation of a Novel Multicompartment Offloader Knee Brace. J. Biomech. Eng. 142, 1–8. https://doi.org/10.1115/1.4044818
- McGibbon, C.A., Brandon, S.C., Bishop, E.L., Biden, E.N., Cowper-Smith, C., 2020. Biomechanical study of a novel tri-compartmental offloader brace for the knee. In Preparation.
- Budarick, A.R., Bishop, E. and Cowper-Smith, C., 2020. Evaluation of a new orthotic for multi-compartment knee osteoarthritis: a retrospective pilot survey. Submitted to Annals of Physical and Rehabilitation Medicine.