
You may have read our Guide to Severe Knee Arthritis to help make sense of what’s happening in your knee as your arthritis gets worse. Now you’re ready for a full overview of the options available to treat and manage your severe pain and loss of mobility. We created this guide to be a simple but comprehensive resource to help you navigate your treatment options and have a more informed conversation with your doctor and other healthcare professionals. Advanced knee arthritis comes with its own unique set of symptoms and challenges. As arthritis causes further degeneration of the knee joint, the space between the bones in the joint narrows, cartilage and meniscus damage increase, synovial fluid decreases and becomes less effective at lubricating your joint, and more bone spurs (also called osteophytes) can develop. With so many factors to consider it’s not surprising that there are many treatment options available. This is a complex topic and can feel overwhelming and confusing, especially given the conflicting information provided by various sources. You just want to know what options are out there, and more importantly, what the best ones are for your advanced knee arthritis. To help you understand the full range of solutions available to you, this user-friendly guide summarizes and ranks the top-recommended treatment options based on a Strength of Recommendation (SOR) score.
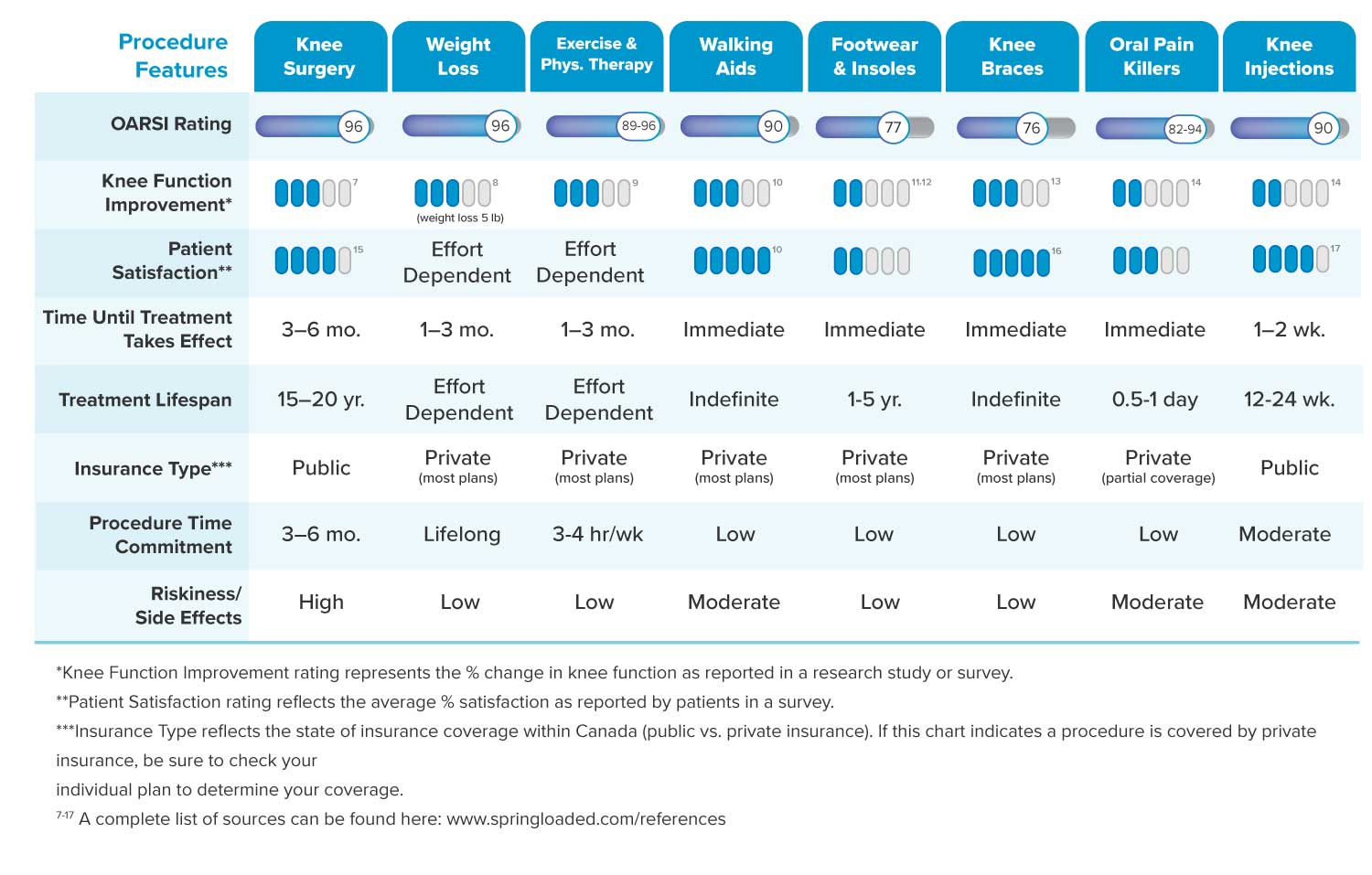
The SOR system was developed by OARSI (Osteoarthritis Research Society International) which assembled an expert committee of specialized hip and knee osteoarthritis healthcare professionals for the task. The scores take into account research evidence for safety, effectiveness, and cost-effectiveness. Management and treatment options are divided into three categories: non-pharmacologic (non-drug), pharmacologic (drug), and surgical treatments. Each treatment has a SOR score represented by a percentage with 0% being the least recommended treatment and 100% the most recommended. As knee arthritis becomes more severe, expert consensus is that a treatment plan will likely include a combination of both pharmacological and non-pharmacological treatments, and what works well for one person may not work well for another. Treatment choices are usually personalized, and will likely include some trial and error until the right combination of solutions is found to successfully manage pain and improve mobility. It’s important to consult with your doctor before making any changes to your current pain and mobility management routine.

Education and Self-management 1
(OARSI Strength of Recommendation Score – 97%) A clear understanding of the objectives behind your treatment – including what success of that particular treatment looks (and feels) like to you, and the importance of making changes to your lifestyle – in terms of identifying and sticking to a treatment plan – was unanimously identified by OARSI experts as the most important place to start. Because each person’s advanced stage knee arthritis looks so different (in terms of both anatomy and symptoms) it’s difficult to say that a single particular treatment is going to be effective for any one person. Expert consensus is also that at your advanced stage, your treatment plan is very likely going to include a combination of both drug-based and non-drug-based treatments. Doing your own research, working with your doctor and other specialists, and some ‘trial and error’ will likely be involved as you uncover which solutions are best for you at this time. It’s important to take the time to ensure you fully understand the problem so that you can work effectively with healthcare professionals to pinpoint the best solutions for you. If you feel like you don’t fully understand what’s happening to your knees as your arthritis progresses, you may want to read our Guide to Advanced Knee Arthritis before you continue reading this guide. Once you are comfortable with the basics you’ll be in a better position to explore the full range of treatment and management options available to you.
Weight Reduction 1-2
(OARSI Strength of Recommendation Score – 96%) Any additional force put on your weight-bearing joints (hips, knees, and ankles) is directly linked to increased pain and inflammation – particularly on the knees. It’s said that when you walk across level ground, the force on your knees is the equivalent of 1½ times your body weight. That means a 200-pound person will have 300 pounds of pressure on their knees with each step. If you add an incline, stairs, or any kind of deep knee bend motion, the forces in your knee can be as high as seven times your body weight. Aside from excess weight creating additional joint pain and discomfort, a number of inflammatory chemical mediators produced in fat can affect joint tissues and can amplify the pain you feel. So by getting rid of any excess fat tissue, not only are you offloading the pressure on your joints, but you could also be eliminating some of the chemicals in your body that intensify that pain. Weight loss for anyone, but especially for those who have mobility limitations, can be a difficult and lengthy process but can have a significant impact in reducing pain. It’s recommended to work with your doctor and other specialists to determine your weight loss goal, and how to safely achieve it.

 Exercise 1,3
Exercise 1,3

(OARSI Strength of Recommendation Score – 96%) While it may sound counterintuitive to exercise a joint that is painful during movement, experts recommend that a regular exercise routine is, in fact, one of the best ways to manage your knee pain. Exercise can help relieve pain from knee arthritis by strengthening the muscles around the joint. Stronger muscles ease the stress placed on the knee joint and can act as shock absorbers, deflecting some of the day-to-day wear and tear caused by activities like walking. A wide range of exercises can improve knee pain, including weight-bearing, low-impact, and water-based workouts. Regularly performing exercises specifically intended for knee arthritis may help improve your function, mobility, and pain. Talk to your doctor before making any changes to your exercise routine, and consider consulting with a physiotherapist about which movements are best suited for you, and when and how to do them.
Walking Aids 1,4

(OARSI Strength of Recommendation Score – 90%) Assistive Walking Devices (AWD) or mobility aids include canes, crutches, scooters, walkers and wheelchairs. As the name suggests, they are designed to assist people with disability or injury to be more mobile and regain independence. Walking aids are often recommended for their ability to provide additional balance and stability by offsetting some of the weight on your knee to the assistant device. As knee osteoarthritis advances, it becomes less likely that using a walking aid on its own will be enough to sufficiently reduce pain. However, used in conjunction with other appropriate treatments, the additional support of an assistive walking device may provide you with more peace of mind when walking due to the added stability. If you think a walking aid may help you, work with your doctor or physiotherapist to ensure you have the right device and to avoid improper or excessive use and further injury.
Physiotherapy1,5
(OARSI Strength of Recommendation Score – 89%) Physiotherapy also known as physical therapy (PT), is the use of mechanical force and movements, manual therapy, exercise therapy, and sometimes electrotherapy to promote better mobility and function in your bones and joints. Through examination, diagnosis, prognosis, physical intervention, and patient education, you can work with your Physiotherapist to personalize your treatment plan to your specific condition, and to the specific results or outcomes you’re looking for, such as increased strength or improved flexibility. In some cases, Physiotherapy may be provided as the primary treatment for knee arthritis, however, at an advanced stage, it most likely would be used in conjunction with other options.
Footwear & Insoles 1
(OARSI Strength of Recommendation Score – 77%) Insoles are an additional piece of material that can either be purchased off the shelf or customized, that you place inside your shoe for a better fit. Special insoles can work to help reduce pain associated with medial compartment (inner) knee osteoarthritis. The insoles, which are known as lateral-wedge insoles, lessen pain by changing the mechanics of the knee. It’s thinner at the instep and thicker at the outer edge of the foot. This helps to redistribute force from the medial compartment to other parts of the knee. The thickness and shape of the lateral-wedge insole can be customized for individual needs. It’s the opinion of experts that every patient with knee arthritis should receive advice concerning appropriate footwear and insoles. However, at your advanced stage, insoles alone are unlikely to be sufficient on their own to manage your pain, especially if your knee has damage to more than just the medial tibiofemoral compartment.
Knee Braces 1,6
(OARSI Strength of Recommendation Score – 76%) For those with uni-compartment knee osteoarthritis, offloader braces are a mechanical intervention designed to reduce pain, improve physical function, and possibly slow disease progression. Up until recently, uni-compartment offloader knee braces – braces designed to transfer stress or pressure from the inside to outside part of the knee or vice versa – was the only option available for knee osteoarthritis braces. Uni-compartment offloader knee braces are often effective at reducing pain, improving stability and helping to diminish the risk of falling for people with arthritis in one tibiofemoral compartment of the knee. However, they are limited in their ability to address arthritis in multiple compartments of the knee. Because over half of people with knee osteoarthritis have damage done to more than just one compartment of the knee, we designed Spring Loaded braces to address this limitation by using a bionic hinge. The bionic hinge allows the brace to reduce pressure in all three compartments of the knee, making them the only tri-compartment offloader braces on the market. Offloader knee braces, made specifically for those with osteoarthritis, usually consist of molded plastic and foam with steel struts used to limit movement to the side. The braces are typically rigid with a hinge and strap system to secure the brace to the leg. Offloader knee braces have been proven to be effective in the management of knee osteoarthritis for pain relief, improved alignment and increased mobility. However, if you have damage done to more than just one compartment of the knee you may want to consider discussing a tri-compartment offloader knee brace with your doctor.
Hot & Cold Therapy 1,7
 (OARSI Strength of Recommendation Score – 64%) Thermotherapy (heat) and cryotherapy (cold) is the application of therapeutic heat or cold to affected joints. By applying heat through heating pads, hot towels, or paraffin wax, the goal is to improve circulation and relax your muscles. Conversely applying cold through cold compresses, frozen gel packs, crushed ice in a plastic bag (or simply a bag of frozen vegetables) is intended to numb the pain, reduce joint swelling, constrict blood vessels, and block nerve impulses to the affected joint. Short (20 minutes) but consistent ice massages have also been shown to improve muscle strength. Heat, cold, ice massages – or a combination of all three – could be a beneficial addition to a pain management routine for improved knee strength, range of motion, and function. It’s important to talk with your doctor about which method is right for you and to determine how long and how often to use each of the treatments.
(OARSI Strength of Recommendation Score – 64%) Thermotherapy (heat) and cryotherapy (cold) is the application of therapeutic heat or cold to affected joints. By applying heat through heating pads, hot towels, or paraffin wax, the goal is to improve circulation and relax your muscles. Conversely applying cold through cold compresses, frozen gel packs, crushed ice in a plastic bag (or simply a bag of frozen vegetables) is intended to numb the pain, reduce joint swelling, constrict blood vessels, and block nerve impulses to the affected joint. Short (20 minutes) but consistent ice massages have also been shown to improve muscle strength. Heat, cold, ice massages – or a combination of all three – could be a beneficial addition to a pain management routine for improved knee strength, range of motion, and function. It’s important to talk with your doctor about which method is right for you and to determine how long and how often to use each of the treatments.
Acupuncture 1,8


(OARSI Strength of Recommendation Score – 59%) Acupuncture is a traditional Chinese medicine where practitioners insert thin needles through the skin to certain depths and at certain points on the body to help control pain and other symptoms. The needles stimulate specific points to help clear energy blockages, improve blood flow and restore overall health and vitality. Research has shown that for some, acupuncture administered in an intensive two to four-week treatment regimen could offer short-term relief for knee pain. Evidence also showed that real acupuncture was more effective than sham acupuncture (placebo acupuncture where needles do not go as deep and are not used at the same points on the body) for relief of pain.
Transcutaneous Electrical Nerve Stimulation 1
(OARSI Strength of Recommendation Score – 58%) Transcutaneous Electrical Nerve Stimulation (TENS) is the use of electric currents – produced by a medical device – to stimulate nerves for therapeutic purposes. Electrodes are placed on the skin in the affected region then slow electrical pulses cause muscles to contract and relax, essentially mimicking passive exercise. While TENS ranks quite low on the recommendations list, some people with advanced knee arthritis have had success when combining TENS into their treatment plan for temporary pain relief.

Oral NSAIDs 1
(OARSI Strength of Recommendation Score – 93%) Orally taken Non-Steroidal Anti Inflammatory Drugs (NSAIDs) are pills or capsules that work to reduce pain, inflammation, and fever through their analgesic (painkilling), and antipyretic (fever-reducing) properties. NSAIDs you would likely be familiar with are aspirin, ibuprofen (Advil, Motrin), and naproxen (Aleve). NSAIDs are designed to prevent the body from producing a natural enzyme called COX2. COX2 is responsible for the production of hormones called prostaglandins, which trigger the pain and inflammation you experience. NSAIDs have been used for decades to treat the pain from arthritis, however experts recommend they should be used at the lowest effective dose and if possible their long-term use should be avoided because of their known side effects including kidney injury, high blood pressure, fluid retention, heart problems, gastrointestinal ulcers, and bleeding.
Acetaminophen 1
(OARSI Strength of Recommendation Score – 92%) Acetaminophen is a drug ingredient found in two classes of both over-the-counter and prescription medicines. Analgesics (pain relievers) is the first class and antipyretics (fever reducers) is the second. Tylenol is an example of a well-known acetaminophen brand. Like NSAIDs, acetaminophen is believed to work by inhibiting an enzyme called COX-2. By doing so, it prevents the brain from releasing chemicals that activate pain receptors. The benefit of acetaminophen is that it isn’t known to cause side effects like stomach ulcers or heart problems – both known side effects of NSAIDs. However, when taken incorrectly acetaminophen can have side effects that include liver damage. While acetaminophen is typically used for mild to moderate pain relief, depending on your specific case and needs it could be beneficial to incorporate into your pain management routine under the guidance and recommendation of your healthcare professional.
Topical NSAIDs and Capsaicin 1

(OARSI Strength of Recommendation Score 85%) Topical NSAIDs include patches, creams, gels, and ointments and work in the same way as orally taken NSAIDs, but are proposed to have a more favorable safety profile due to the low blood serum concentrations achieved with topical formulations. Topically applied medications reduce pain and inflammation by blocking the production of enzymes that produce inflammatory chemicals that ultimately result in pain and swelling. The pain-relieving property of capsaicin is found in many topical preparations and is known to relieve muscle, joint, and nerve pain. Capsaicin works by desensitizing nerves and blocking pain messages from being relayed to the brain. Topical treatments have been shown to be effective for knee arthritis pain as an adjunctive or alternative treatment therapy. While gastrointestinal side effects are less likely than they are with oral NSAIDs, local reactions such as itching, burning, and rashes are more frequent. It’s important to work with your healthcare professional to ensure you’re using the right solution, strength and application method of the topical treatment.
Narcotic Analgesics (Weak Opioids) 1

(OARSI Strength of Recommendation Score – 82%) Narcotic Analgesics are a class of drug used to relieve pain. Analgesics are broadly categorized as being either non-opioid (non-narcotic e.g. Tylenol) or opioid (narcotic e.g. codeine) pain relievers. Weak opioids include codeine, tramadol and propoxyphene and just like NSAIDs and acetaminophen, they work to relieve pain by blocking pain signals to the brain. Experts advise that the use of narcotic analgesics be considered as a part of your treatment plan where other medications have been ineffective. In some cases though, benefits associated with the use of narcotic analgesics may be outweighed by the side effects including nausea, constipation, dizziness, drowsiness, vomiting and in some cases addiction. Taking any kind of narcotic analgesics should be done under close supervision of your doctor.
Corticosteroids Injections 1,9

(OARSI Strength of Recommendation Score – 78%) Cortisone injections are steroid injections used to reduce joint inflammation. Steroids are synthetic drugs that act like the naturally occurring hormone hydrocortisone, or cortisol. Steroid injections deliver a concentrated dose of medication directly into the affected joint. Corticosteroids work to decrease inflammation as well as harmful autoimmune activity. This means that they reduce the activity of your immune system so that it doesn’t start attacking the tissues and organs of your own body. Experts emphasize the importance of accurate placement of injections to maximize benefit and reduce the risk of side effects. While corticosteroid injections have been shown to reduce inflammation in knee osteoarthritis, there is some evidence to show that the benefits of these injections may not outweigh the negative side effects, one of which is accelerating cartilage damage.
Hyaluronic Acid (Hyaluronan) Injections 1
(OARSI Strength of Recommendation Score – 64%) A normal knee joint is surrounded by a membrane, the synovium, which produces a small amount of thick fluid, known as synovial fluid. Synovial fluid helps to nourish the cartilage and keep it slippery. The synovium also has a tough outer layer (the joint capsule) which protects and supports the joint. In osteoarthritis, as cartilage wears away, synovial fluid changes and loses its ability to lubricate the joint. The treatment, which involves injecting hyaluronic acid into the knee (also known as viscosupplementation) works to improve the lubrication of the knee, reduce pain, and improve range of motion. Typically, hyaluronic acid injections are recommended for patients who have not found adequate pain relief from more conservative treatment options.
Glucosamine and/or Chondroitin Sulfate 1
(OARSI Strength of Recommendation Score – 63%) Glucosamine is a compound found naturally in the body, made from glucose and the amino acid glutamine. Glucosamine is needed to produce glycosaminoglycan, a molecule used in the formation and repair of cartilage and other body tissues. Since the production of glucosamine slows with age, some people use glucosamine supplements to fight aging-related health conditions, like osteoarthritis. Taking glucosamine as a nutritional supplement is thought to keep osteoarthritis in check by restoring the body’s glucosamine supply and repairing damaged cartilage. Treatment with glucosamine and/or chondroitin sulphate may provide symptomatic benefit, however if no response is apparent within 6 months, experts recommend to discontinue treatment.
If your knee function and the severity of your knee pain cannot be managed through a combination of non-pharmacologic and pharmacologic treatments, surgery may be considered.
Total Knee Replacement1
(OARSI Strength of Recommendation Score – 96%) Total knee replacement surgery also referred to as arthroplasty or total joint replacement, is a surgical procedure to resurface a knee damaged by arthritis. Metal and plastic parts are used to cap the ends of the bones that form the knee joint, along with the kneecap. This surgery may be considered for someone who has severe arthritis and hasn’t found relief through medication or non-pharmacologic treatments. During surgery, damaged cartilage and a portion of underlying bone are replaced with a prosthetic knee joint. In other words, an Orthopaedic surgeon removes the damaged joint and puts in a new, artificial one. Theoretically, any joint in the body can be replaced, but most joint replacement surgeries involve the knee and hip. A knee prosthesis (artificial knee) can be made out of metal and/or plastic, it also can be cemented with a grout-like substance, non-cemented, or a combination of both to achieve fixation. Typically a cemented prosthesis is used for those at your advanced stage. Total knee replacement surgery has been proven to be effective in reducing pain and restoring function to the joint for those experiencing severe symptoms. The benefits from surgery can last up to 20 years, but a total knee replacement surgery is often only considered as a last resort treatment option when pain is no longer well-controlled and joint damage significantly affects quality of life. Other considerations that should be discussed with your doctor include whether or not you qualify for the surgery, wait times and cost for surgery and recovery time.
 Partial (Uni-compartmental) Knee Replacement 1,10
Partial (Uni-compartmental) Knee Replacement 1,10

(OARSI Strength of Recommendation Score – 76%) Like total knee replacement surgery, partial or uni-compartment knee replacement surgery is a surgical procedure to resurface a knee damaged by arthritis to reduce pain and improve function. However, unlike a total knee replacement surgery, a partial knee replacement is only performed when damage exists in one compartment of the knee. During the procedure, your surgeon removes the cartilage from the damaged compartment of your knee and then replaces that cartilage and bone with metal coverings that recreate the surface of the joint. Just like in a total knee replacement, these metal parts are typically held to the bone with cement. To finish the procedure a plastic insert is placed between the two metal components to create a smooth gliding surface. The benefits of a partial knee replacement surgery are that it’s less invasive than a total knee replacement surgery and has a quicker recovery time. Also, because healthy parts of your knee are left in place, partial knee replacements are said to feel more natural than a total knee replacement. Downsides of a partial knee replacement are that another surgery (total knee replacement) may be needed in the future if damage to another compartment occurs. Also, because over half of people with knee osteoarthritis have damage and deterioration to more than just one compartment of the knee, fewer people are good candidates for this surgery.
Osteotomy 1,12-14
(OARSI Strength of Recommendation Score – 75%) Osteotomy is a surgical procedure meant to preserve the joint, where the surgeon removes a wedge of bone located near the damaged joint. The goal of the surgery is to help correct poor knee alignment and to prolong the lifespan of the knee joint. The procedure is meant to cause a shift of weight from the area where there is cartilage damage to an area where there is more normal or healthy cartilage. In osteoarthritis, the damage is typically more significant on the inner portion of the knee, so the surgeon removes bone from the outside of the lower leg bone near the knee. Ultimately, this allows the weight to be distributed more evenly across the joint cartilage. While osteotomy is oftentimes successful in relieving pain and delaying the progression of arthritis, the surgery is typically only performed on people under the age of 60 with earlier stage symptoms and where damage has only been done to one side of the knee joint. While benefits from osteotomy surgeries have been known to last over 15 years in a lot of cases if deterioration occurs in other compartments of the knee another surgery could be needed. It has been shown that when an osteotomy for medial compartment arthrosis is performed in an otherwise healthy knee, no degenerative changes occur in the lateral or patellofemoral compartments. On the other hand, an osteotomy does not manage symptoms related to bicompartmental or tri-compartment arthrosis of the knee.

Approximately 15% of the world’s population has OA.19 With a staggering 630 million suffering from OA it is increasingly becoming a burden on healthcare systems. Consequently, many scientists and engineers have been hard at work developing cost-effective alternatives to knee replacement surgeries. Recently two promising innovative approaches have been gaining popularity for the treatment of severe knee OA
- Knee exoskeletons and bionics artificially enhance knee strength while simultaneously offloading the entire joint.
- Stem cell therapy aims to help patients increase the regenerative capacity of their own joint tissue.
Knee Bionics & Exoskeletons
Bionics and exoskeletons augment joint function by enhancing your strength above and beyond what your body could produce naturally in an unassisted manner. You can think about these devices as instantly adding extra muscle mass to your legs. Products in this category typically have motorized, pneumatic and/or spring hinges that provide a dual benefit as they not only increase the strength of the knee but they also provide joint distraction – offloading all three compartments of the knee joint. Tri-compartment offloading has been identified by healthcare professionals as a best practice for the conservative management of osteoarthritis. Further, reducing the compressive force on the knee joint is also the focal point of weight loss and dieting – a gold standard treatment for Osteoarthritis. A recent study showed that knee bionics can reduce compression forces across the joint by over 40%.20 This is a significant advancement over traditional knee braces that do not enhance strength and are only able to offload one compartment at a time. Since over half of OA patients have degenerative changes in more than one compartment of the knee, these technologies can be particularly effective for the majority of individuals suffering from moderate-severe osteoarthritis.21
Another advantage of these technologies is that they are low risk and the results can be realized immediately. Exercise and weight loss, while effective in increasing joint function and reducing pain, must be maintained over a long period of time to see any benefit. When you don a knee exoskeleton or bionic brace, you can immediately start performing activities that were once limiting and painful.
Active Exoskeletons vs Passive Exoskeletons
There are a variety of exoskeletons and bionic devices on the market today. A key distinction between these products is whether or not they use robotic and electronic components. Motorized units are called active exoskeletons because they provide external assistance that does not rely on body movement to bring energy into the system. Passive exoskeletons typically use the kinetic energy produced by normal body movement to provide extra assistance. The latter is usually much less expensive ($1000 – 5000), lighter in weight, and requires the user to have some level of baseline physical function. An active exoskeleton can cost upwards of $40,000 and is appropriate for individuals suffering from extreme neurological deficits where they are unable to move their limbs.
Stem Cell Therapy
You’ve probably heard about Stem Cell therapy before. While treatment purveyors have received some negative press it doesn’t diminish the fact that stem cells have a wide range of applications including osteoarthritis. While still in the early stages of scientific research, preliminary results are encouraging. Stem cells can be thought of as unspecialized multi-purpose cells. They are distributed in a variety of locations all over the human body and have the ability to transform into other cell types that are beneficial to specific tissues.
The cartilage degradation in osteoarthritis is characterized by negative changes in collagen metabolism. Rather than continually growing new collagen cells, which maintain the cushioning between the surfaces of your knee joint, the growth cycle is interrupted and collagen is replaced at a lower rate. This is the crux of degenerative joint disease. Stem cells are thought to be able to benefit this problem at the source by transforming into pro-collagen cells that support the rebuilding of healthy tissue in the area. The hope is that this therapy could help regrow healthy tissue in the knee, and allow individuals to avoid or delay getting knee replacement surgery. Stem cells can be transferred to damaged areas of the joint with both surgical and non-surgical means.
Surgical (Scaffolding Techniques)22
The central limitation of surgical techniques is that they only affect specific areas of the joint surface targeted by the surgery while neglecting the joint globally. Therefore they likely have limited efficacy for patients suffering from advanced osteoarthritis where multiple compartments of the joint are affected. The procedures are also not considered long term solutions.
Autologous Chondrocyte or MSC Transplantation: Cartilaginous tissue from a healthy/non-weight bearing area of the joint is extracted, cultured and then patched over top of an area of the joint where cartilage has disappeared. Early results are encouraging showing cartilage growth and renewal, however, it is an invasive surgery and larger studies are required to confirm its efficacy.
Microfracture Surgery (Osteoplasty): A procedure that primarily involves drilling into the bone near areas where cartilage has degraded. Because bone marrow is rich in stem cells, they are thought to leak into the surrounding joint capsule helping rebuild cartilage. Non-Surgical (Injections)22
Injectable Stem Cells
Stem cells harvested from blood, fat, or bone tissue are injected into the affected knee joint. This procedure is less invasive than surgical stem cell treatments and has been shown to significantly improve knee function. That being said, evidence regarding tissue regeneration after these injections remains inconsistent. Additionally, after treatment is complete it is difficult to predict when any therapeutic benefits will be realized.
Bone marrow or adipose tissue stem cell therapy can cost anywhere between $5000-10,000 in the US.23 While stem cell injection therapy shows promise, consumers should remain cautious. A number of clinics have been caught claiming to sell stem cell therapies despite using unrelated substances that could put patients at risk.
| If you are not a great candidate for surgery (see more here) or just wish to avoid it for personal reasons – Exoskeletons, Bionics, and Stem Cell Therapies could provide you a viable, less invasive alternative. |
Now that you have a complete overview of the standard and new treatments available for knee osteoarthritis it’s time to delve a little deeper into your options. Every treatment has tradeoffs, so at this point, a thorough cost-benefit analysis is necessary in order to allow you to make decisions about your future health with absolute confidence. Generally, it is recommended to exhaust your conservative treatment options before considering surgical or invasive pharmacological alternatives. This is because, while effective, the side effects and potential complications are higher with these options making them more of a last resort for patients who are typically older and have extremely debilitating symptoms.
| The American Osteopathic Association recommends considering surgery only for those who still have significant knee pain following a minimum of 6 months of conservative treatment and exploring different options for non-surgical management.24 |

Surgical
Am I a Good Candidate?
- In order to be considered a good candidate for knee replacement surgery, researchers suggest that you should meet specific criteria pertaining to your symptoms, disease state, and age.
- Another factor that can influence the viability of surgery is the presence of other health conditions also known as ‘comorbidities’. Diabetes, High Blood Pressure and Obesity are the most common. If you have one or more of these conditions, the risks associated with the surgery itself and the recovery could be higher.
- If you are Canadian, one of the main considerations you may have is the wait time for the surgery which can be over six months depending on the area you reside in. Even then, In some locations, only 41% of patients receive their surgery within six months.
How Long Does it Take to Recover From Surgery?
People are often able to walk within days after the surgery so the recovery time can be quite short. Recovery time varies among people and their level of health before surgery can play a large role in the amount of recovery time that may be needed. For more information on surgery recovery times check out our blog post about timelines for recovering from knee replacement surgery!
How Much Does Knee Replacement Surgery Cost?
In Canada, the cost of the knee replacement surgery is covered through Medicare but in the United States the price averages around 50,000 USD. Due to the prohibitively high cost, many uninsured or underinsured people who would be perfect candidates are unable to afford the surgery or they wait until there are no options left.
Benefits of Surgery
A total knee replacement surgery is considered an effective method for relieving the symptoms of severe osteoarthritis in the affected joint. The affected parts of the bone in the area are completely removed so it can drastically reduce pain and increase mobility as the diseased bone is removed. Another benefit is that there is often a relatively short recovery time and as previously mentioned the artificial knee joint can last upwards of 20 years.26 The primary objective of knee replacement surgery is to allow patients to perform activities of daily living (ADL) without pain. More information about ADLs and knee surgery.
Management of Expectations
One common misconception with total knee replacements is that they will restore function to a level similar to what they would have had before the onset of osteoarthritis. While the surgery is undoubtedly one of the best ways to relieve severe osteoarthritis symptoms it cannot restore function to that level at this point in time.27
Five years after having a total knee replacement patients report a slight decrease in sport participation, and out of those that participated in sporting activities greater than 2 hours decreased from 12.0% to 5.0%.28 Physically demanding occupations like sports may also be affected. A study on military service members showed that 18% of active service members were unable to return to active duty after their operation.29
One of the major benefits of undergoing a total knee replacement is the increased joint range of motion. However that being said, most patients exhibit a functional deficit in knee range of motion at 18 months post-surgery. This means that despite having better knee joint flexibility, they are still reluctant to squat deeply or kneel down. The ongoing deficit has been attributed to a continued lack of stability and strength around the joint which causes movements that involve a deep knee bend (squatting, lunging, etc.) to feel unstable.30
Surgery Complications
One of the drawbacks of undergoing a knee replacement is that while the surgery is relatively safe it still carries risks. Of all knee replacement surgeries carried out in Canada (2016) 7.6% required revision surgery for complications including infection, instability or aseptic loosening (failed bonding between bone and the artificial implant)25
Reasons for Revision
Revision surgery is sometimes necessary for patients who undergo total knee replacements. In this section, we will discuss the most common culprits and what they entail. The most common reasons for revision were aseptic loosening (28.7%), infection (23.4%) and instability (15.9%).31
Instability of Artificial Knee Joint
Instability of the artificial knee joint is responsible for revision in about 7%-30% of surgeries. Instability is defined as abnormal movement of the artificial joint followed by clinical failure. 31 When diagnosing instability of the joint is important to rule out other causes of the symptoms like infection before the corrective surgery takes place. In most cases, instability is preventable by good surgical technique as well as proper selection of a prosthesis.
Infection
There is a risk of infection associated with artificial knee replacements with approximately 1 in 100 people contracting infections after the surgery.32 Common ways for bacteria to enter the body are cuts in the skin, major dental procedures and through wounds during other surgical procedures. Common symptoms of infection of the joint are pain, swelling, redness, warmth at the joint, and fever. If the infection is diagnosed early enough the chances are higher that revision surgery will not be needed.
Aseptic Loosening
It can occur 10-20 years after receiving a TKR when debris from the wear of the artificial joint triggers a response from the body’s immune system causing inflammation and damage to the joint. The immune system is triggered by microscopic pieces of the artificial joint that break off during normal wear over years of use. The immune system responds to the “foreign bodies” in the same way as it fights off diseases but unfortunately, in this case, it leads to Osteolysis (pathological destruction of bone tissue) as the body reabsorbs the bone tissue to try and repair the perceived damage.33
Pharmacologic
The most commonly prescribed family of drugs in the management of Osteoarthritis are NSAIDs. These drugs range from over the counter medications like ibuprofen, to more powerful prescription drugs like celecoxib (Celebrex). They are widely available, fast-acting, and generally well tolerated. However, continued long term use of these drugs comes with significant risks.
- NSAID use in patients aged >65 years more than doubles the risk of acute kidney injury in the next 30 days.34
- NSAIDs increase fluid retention and blood pressure by an average of 5 mmHg.34
- High doses of NSAIDs cause 7-9 non-fatal and 2 fatal cardiovascular events per 1000 patients annually.34
- Regular NSAID use increases the risk of Gastrointestinal bleeding 4-fold.34
Topical NSAIDs can reduce some of the risks for gastrointestinal side effects associated with oral NSAIDs while providing similar pain-relieving benefits. However, they come with an increased risk of dry skin, rashes, and itches at the site of application.35
Acetaminophen, commonly known as Tylenol or Aspirin offers slightly less relief in symptoms as compared to NSAIDs. The possible side effects associated with long term use are less severe, although regular use of this class of drugs can cause elevated liver enzymes, a sign of liver toxicity.35
The bottom line is that painkilling drugs do not appear to be a long term solution. Rather it is recommended that be used to manage pain flare-ups where necessary. Regular use should be avoided over long periods of time.
Your Osteoarthritis Treatment Strategy
After reading this guide you should have a general understanding regarding the array of available treatments for severe osteoarthritis, the best practices suggested by researchers and physicians, and an understanding of the costs and benefits associated with surgical and pharmacological management. Keep in mind that there is no single “best” treatment for osteoarthritis. It all depends on your lifestyle and goals. Always try to think about your treatment decision in terms of sustainable solutions that support your future objectives.
What’s Next?
- If surgery is something that you are seriously considering check out Five Thing to Consider Before Knee Surgery to ensure you have all the information you need to maximize your recovery and final outcome.
- If you want to avoid surgery and reliance of pain-killing drugs visit the Conservative Treatment Guide and begin determining what treatment plan will fit your lifestyle and goals.
References
- W. Zhang et al., OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis and Cartilage, 2008.
- Why weight matters when it comes to joint pain, Harvard Medical School.
- Tammy C. Hoffmann et all, CMAJ, Prescribing exercise interventions for patients with chronic conditions, 2016.
- Laura D. Carbone, MD, MS, et all, Assistive Walking Device Use and Knee Osteoarthritis: the Health, Aging, and Body Composition Study (Health ABC Study), Arch Phys Med Rehabil. 2013 Feb; 94(2): 332–339.
- Anne Ahlman, MPT, Pathway to Independence: Physical Therapy for Patients With Rheumatoid Arthritis, MedGenMed. 2004; 6(2): 9.
- Dan K. Ramsey, PhD, Mary E. Russell, MS, Offloader Braces for Medial Compartment Knee Osteoarthritis Implications on Mediating Progression, Sports Health. 2009 Sep; 1(5): 416–426.
- Brosseau L1, Yonge KA, Robinson V, Marchand S, Judd M, Wells G, Tugwell P., Thermotherapy for treatment of osteoarthritis.,Cochrane Database Syst Rev. 2003;(4):CD004522.
- Daniel Pendick, Acupuncture for knee arthritis fails one test but may still be worth a try, Harvard Medical School, 2014.
- Kirstie Saltsman, Ph.D., Long-term Benefit of Steroid Injections for Knee Osteoarthritis Challenged, National Institutes of Health, 2017.
- Jared R. H. Foran, MD, Unicompartmental Knee Replacement, The American Academy of Orthopaedic Surgeons, 2016.
- Paul A. Manner, MD, Jared R.H. Foran, MD, Osteotomy of the Knee, The American Academy of Orthopaedic Surgeons, 2017.
- Abhay Tillu, Sumedha Tillu, Sarah Vowler, ACUPUNCTURE IN MEDICINE, Effect of Acupuncture on Knee Function in Advanced Osteoarthritis of the Knee: A Prospective, Non-Randomised Controlled Study, 2002;20(1):19-21.
- Peri J. Ballantyne Monique A. M. Gignac Gillian A. Hawker, the American College of Rheumatology, A patient‐centered perspective on surgery avoidance for hip or knee arthritis: Lessons for the future, Arthritis Care and Research: 15 February 2007, 27-34.
- G. Papachristou et all, Deterioration of long-term results following high tibial osteotomy in patients under 60 years of age, Int Orthop. 2006 Oct; 30(5): 403–408.
- Federico Dettoni, MD, et all, HIGH TIBIAL OSTEOTOMY VERSUS UNICOMPARTMENTAL KNEE ARTHROPLASTY FOR MEDIAL COMPARTMENT ARTHROSIS OF THE KNEE: A REVIEW OF THE LITERATURE, Iowa Orthop J. 2010; 30: 131–140.
- Jared R. H. Foran, MD, Unicompartmental Knee Replacement, The American Academy of Orthopaedic Surgeons, 2016.
- Dr. Sarah Ward, MD, FRCSC, Knee Replacement Surgery, The Arthritis Society, 2017.
- Knee Exercises, The American Academy of Orthopaedic Surgeons, 2009.
- Osteoarthritis Research. Retrieved from: https://www.hss.edu/osteoarthritis-research.asp
- McGibbon, C. & Mohamed, A. Knee Load Reduction From an Energy Storing Mechanical Brace. Canadian Society for Biomechanics (2018)
- Shahid, M.K., Al-Obaedi, O., Shah, M. Prevalence of Compartmental Osteoarthritis of the Knee in an Adult Patient Population: A Retrospective Observational Study
- Freitag, J., Bates, D., Boyd, R., Shah, K., Barnard, A., Huguenin, L., & Tenen, A. (2016). Mesenchymal stem cell therapy in the treatment of osteoarthritis: reparative pathways, safety and efficacy–a review. BMC musculoskeletal disorders, 17(1), 230
- Cost of Stem Cell Treatments. Retrieved from: https://bioinformant.com/cost-of-stem-cell-therapy/
- Van Manen, M. D., Nace, J., & Mont, M. A. (2012). Management of primary knee osteoarthritis and indications for total knee arthroplasty for general practitioners. The Journal of the American Osteopathic Association, 112(11), 709-715.
- Canadian Institute for Health Information. Canadian Joint Replacement Registry Annual Report. Retrieved from: https://secure.cihi.ca/free_products/cjrr-annual-report-2018-en.pdf
- Arthritis Research UK. How long will a knee replacement last? Retrieved from: https://www.arthritisresearchuk.org/arthritis-information/surgery/knee-replacement/how-long-will-it-last.aspx
- American Academy of Orthopaedic Surgeons: Preparing for joint replacement surgery. Retrieved from: https://orthoinfo.aaos.org/en/treatment/preparing-for-joint-replacement-surgery/
- Huch, K., Müller, K. A. C., Stuermer, T., Brenner, H., Puhl, W., & Guenther, K. P. (2005). Sports activities 5 years after total knee or hip arthroplasty: the Ulm Osteoarthritis Study. Annals of the rheumatic diseases, 64(12), 1715-1720.
- Belmont Jr, P. J., Heida, K., Keeney, J. A., Hamilton, W., Burks, R., & Waterman, B. R. (2015). Return to work and functional outcomes following primary total knee arthroplasty in US military service members. The Journal of arthroplasty, 30(6), 968-972.
- McClelland, J. A., Feller, J. A., Menz, H. B., & Webster, K. E. (2017). Patients with total knee arthroplasty do not use all of their available range of knee flexion during functional activities. Clinical Biomechanics, 43, 74–78.doi:10.1016/j.clinbiomech.2017.01.022
- Chang, M. J., Lim, H., Lee, N. R., & Moon, Y. W. (2014). Diagnosis, causes and treatments of instability following total knee arthroplasty. Knee surgery & related research, 26(2), 61.
- American Academy of Orthopaedic Surgeons: Knee Replacement Treatment. Retrieved from: https://orthoinfo.aaos.org/en/treatment/total-knee-replacement/
- Abu-Amer, Y., Darwech, I., & Clohisy, J. C. (2007). Aseptic loosening of total joint replacements: mechanisms underlying osteolysis and potential therapies. Arthritis research & therapy, 9(1), S6.
- Davis, A., & Robson, J. (2016). The dangers of NSAIDs: look both ways.
- for Clinical, J. M. E. C. (2012). Analgesics for Osteoarthritis. In Comparative Effectiveness Review Summary Guides for Clinicians [Internet]. Agency for Healthcare Research and Quality (US).