
Introduction
You’re here because your knee, either due to a sudden injury, chronic condition or regular wear and tear is causing you pain. You’re also not alone, 25% of adults suffer from regular bouts of knee pain.1,2 Doctors visits related to knee pain have risen 60% over the last 25 years.2 The knee joint is particularly at risk for injury and aggravation, as even during walking it is subjected to 3 times your bodyweight in pressure.3 Knee pain going down stairs, climbing stairs, squatting, jogging, and playing sports is often more intense due to even greater strain on your knees. All this being said, returning your knees to a strong and healthy state is crucial for your quality of life. How and what you should do from here all depends on understanding the root cause of your knee pain.
What is “ Knee Pain”?
Believe it or not, pain is actually a good thing for the most part. It is a natural signal that our body produces for specific reasons. There are three main types.4
- Nociceptive Pain: Ever actually touch a hot stove when you were young? This is nociceptive pain. It is reactionary by nature – you feel an intense sensation of pain and automatically withdraw from it as quickly as possible. The system of receptors in our skin and other cells helps prevent us from damaging ourselves by increasing our sensitivity to dangerous objects in our environment.
- Inflammatory Pain: Managed by our immune system, inflammatory pain typically comes after an initial injury. Swelling, redness, puffiness, tenderness, soreness, stiffness, are all symptoms that we associate with this type of pain. It can actually be helpful as initially, it discourages movement of the injured area, allowing the body time to heal. Over time this type of pain typically decreases and disappears.
- Pathological Pain: This type of pain is not helpful, and arises when the nervous system keeps producing inflammation despite the absence of an actual injury. This is considered a disease of the nervous system. Another way of describing this is would be a “failed healing response”.
If pain were a fire alarm, nociceptive pain would be the equivalent of a fire alarm going off in response to intense heat. Inflammatory pain would be a reaction to warm temperatures. Pathological pain would be considered a malfunctioning fire alarm sounding randomly despite normal temperatures.
Inflammatory knee pain can either sneak up on you slowly or be the result of an acute injury. This is often the first clue in diagnosing a knee injury, pain that arises slowly is associated with the development of arthritis, while sudden pain is associated with traumatic injuries like ligament tears.

Knee Pain Location & Anatomy
Where on or in your knee are you feeling your pain? This an important clue as to what structures are damaged due to arthritis, injury, or other disorders. In relating the location of your pain to the damaged joint structure, it is helpful to have an understanding of knee anatomy.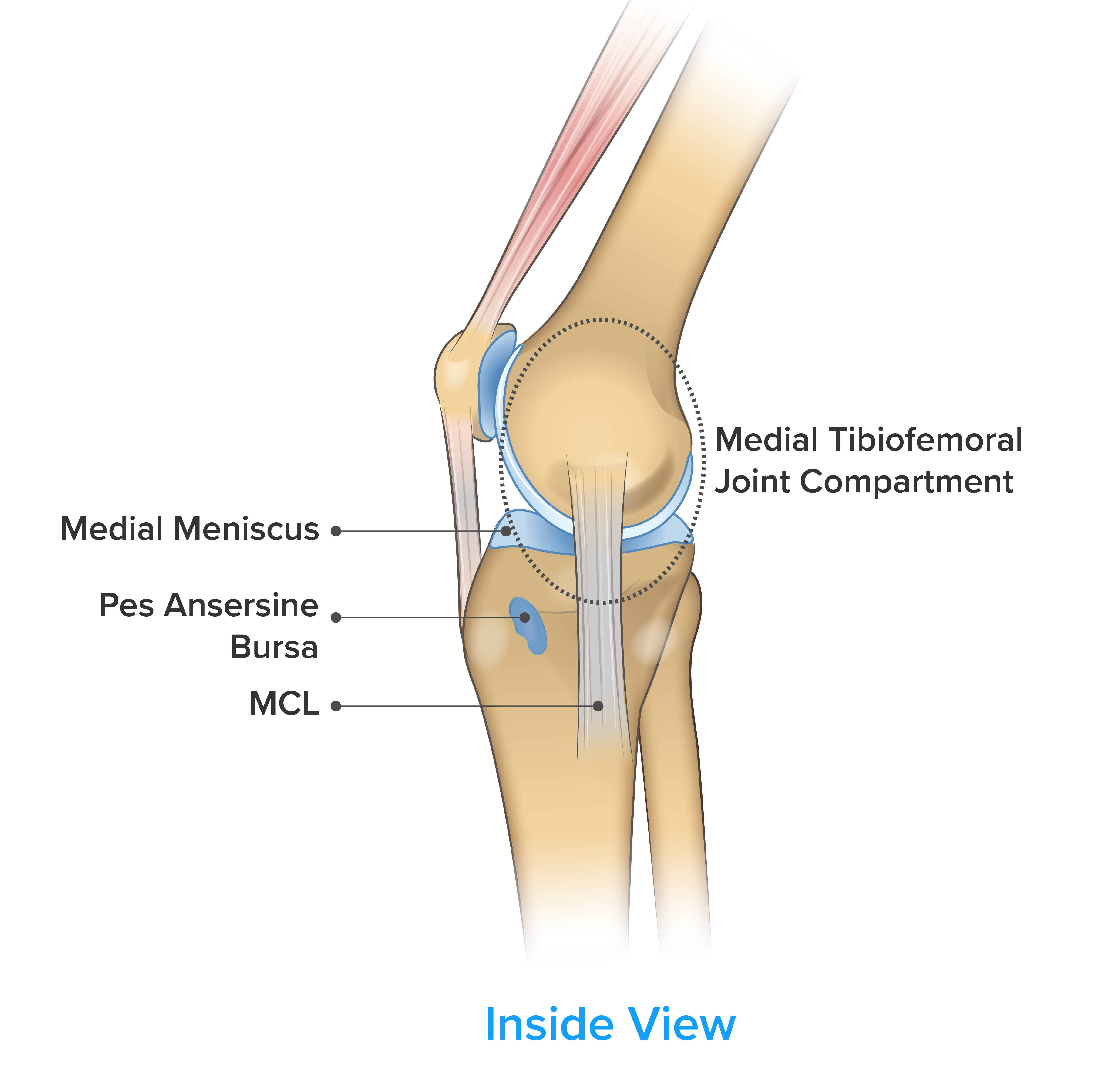
Symptom: Knee pain on the inside of the knee.
- Medial Collateral Ligament (MCL): This ligament is commonly strained or ruptured playing sports – typically during twisting or cutting movements.
- Medial Meniscus: This tissue provides cushioning for your knee joint, and is often injured playing sports and can be damaged through repetitive high load movement like squatting and lunging. “Knock knee” individuals are at high risk of injuring this structure.
- Medial Joint Compartment: One of the common areas for osteoarthritis. Arthritis typically occurs here as you get older. Previous knee injuries also put you at higher risk.
- Pes Anserine Bursa: A condition called bursitis is caused by inflammation of this area due to repetitive stress. Pain is localized slightly below the knee joint on the shin bone.
Pain on the inside of the knee is one of the common joint pain-related complaints. For an in-depth guide on this topic check out: Knee Pain on the Inside of the Joint.
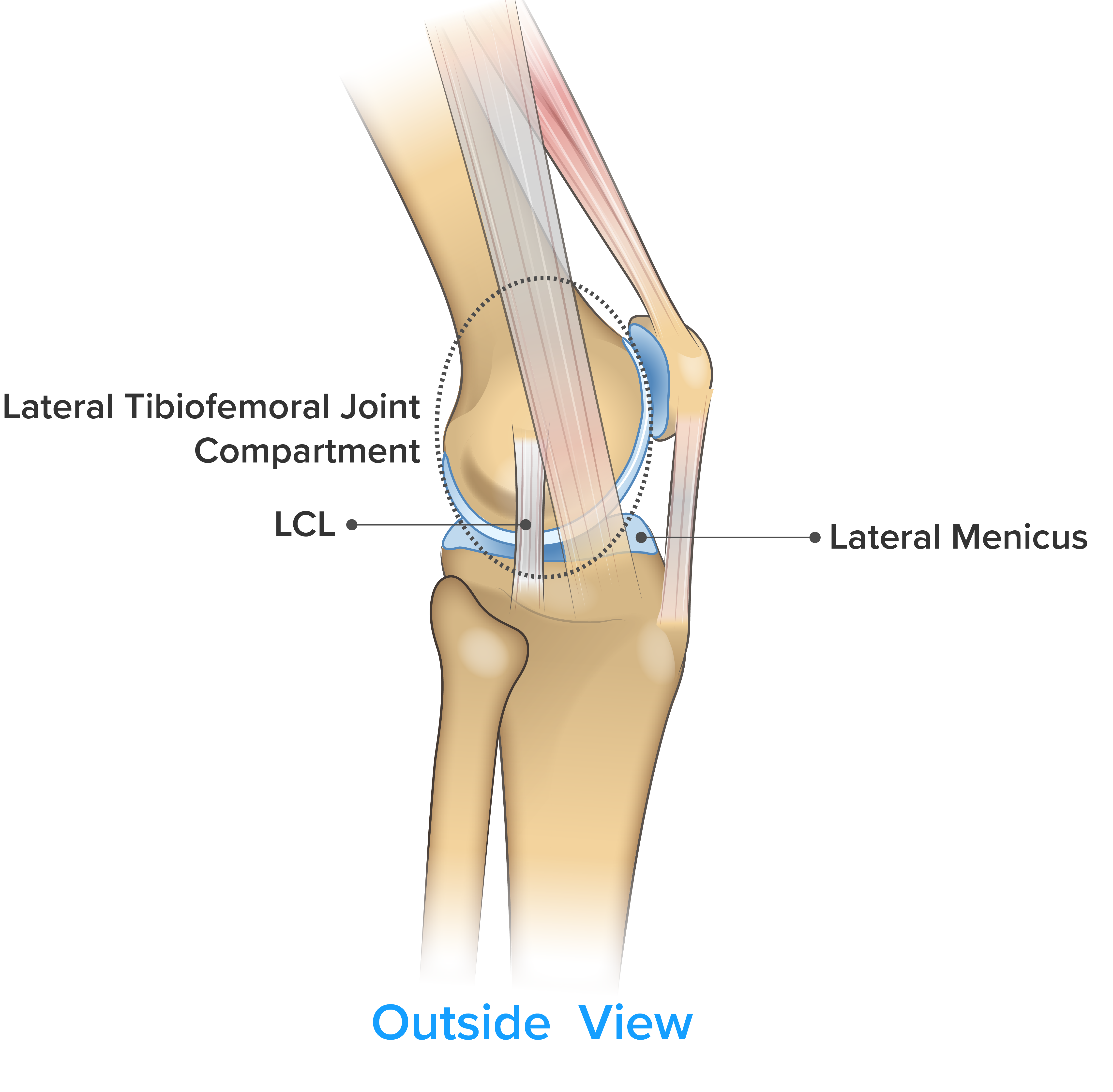
Symptom: Knee pain on the outside of the knee.
- Lateral Collateral Ligament (LCL): This ligament is commonly strained or ruptured playing sports – typically during twisting or cutting movements.
- Lateral Meniscus: This tissue provides cushioning for the outside of your knee joint, and is often injured playing sports. It can be damaged through repetitive high load movements like squatting and lunging. Bow-legged individuals are at higher risk of injuring this structure leading to pain on the outside of the knee.
- Lateral Joint Compartment: Arthritis commonly occurs between the lateral end of your shin and thigh bone. Pain on the outside of the knee (lateral) from arthritis is less common than pain on the inside of the knee (medial).
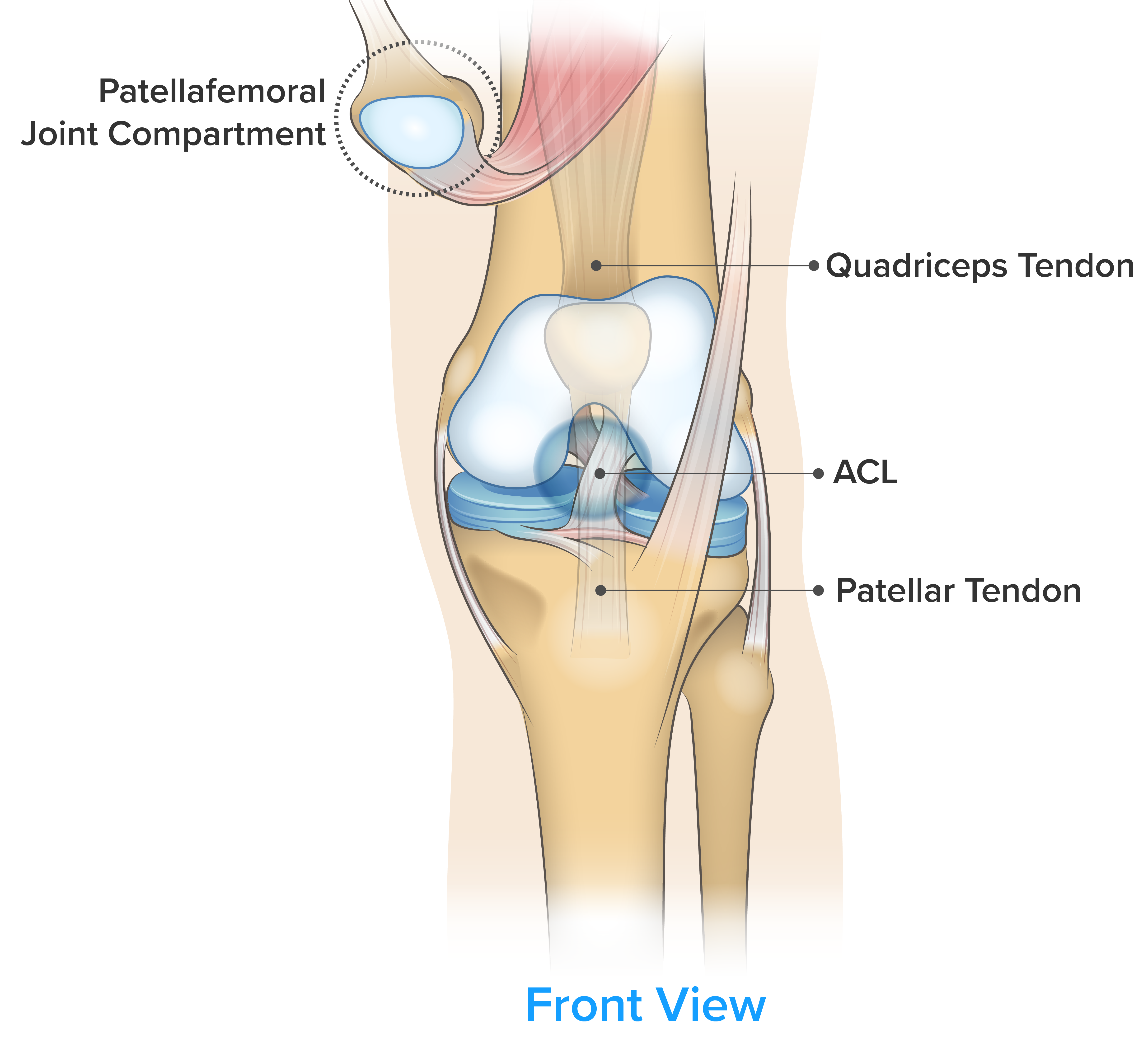
Symptom: Knee pain on the front of the knee.
- Anterior Collateral Ligament (ACL): This ligament is commonly strained or ruptured playing sports – typically during twisting or cutting movements.
- Tendons:
- Patellar Tendonitis: Typically, this injury is only seen in athletes who play sports that require frequent jumping.
- Quadriceps Tendonitis: Typically, seen in individuals who perform excessive deep squatting movements.
- Patellar Joint Compartment:
- Patellar Arthritis: Arthritis commonly occurs under the kneecap. Typically aggravated during activities that require a deep knee bend.
- Patellofemoral Disorder: Caused by improper tracking of the kneecap during movement.

Symptom: Knee pain on the back of the knee.
- Posterior Collateral Ligament (PCL): This ligament is commonly strained or ruptured playing sports – typically during twisting or cutting movements.
- Popliteal Muscle: A small muscle on the back of the knee that helps with extension. When injured, climbing stairs and jogging could be painful.
- Popliteal Bursa: Excessive fluid buildup in the back of the knee can cause this fat pad to swell up. Often a large bulge will appear causing pain with compression and deep knee bending.
Other Knee Pain Related Symptoms
Symptom: Cannot Straighten Knee
- This is most commonly associated with a meniscus injury. Typically a sensation of pressure develops as the knee extends, limiting the range of motion. Range of motion is usually restored with rest and an exercise regime geared towards knee flexibility and stability.
Symptom: Cracking & Popping Sounds (Crepitus)
- Cracking and popping noises (crepitus) while bending your knee are considered normal and on their own shouldn’t be cause for alarm. However, if you are also experiencing “grinding” sensations and pain it may be a sign that the cartilage in your knee is becoming worn. One of the earliest signs of patellofemoral osteoarthritis is painful crepitus.5 In this case, it is worth talking with your doctor to get ahead of what is a progressive degenerative knee disorder.
Symptom: Poor Balance & Instability
- Do you feel uneasy crossing rough terrain or walking up and down stairs? This is likely the result of muscle weakness and proprioceptive (balance) deficits. Both are common during and after an initial injury. An experienced personal trainer or physical therapist can provide you with guidance and tailor a program to fit your needs.
Knee Pain when Exercising
Sometimes your knee will start bothering you despite having never explicitly injured it. When knee pain is not consistent and occurs only during specific activities – Degenerative disorders and overuse injuries are often the culprit.
Symptom: Knee pain when walking
- If you have noticed that your knees are painful when walking it could be a sign that you are developing tibiofemoral osteoarthritis. Arthritis on the inside of your knee (Medial tibiofemoral arthritis) is more than 3 times as common compared to the outside (lateral tibiofemoral arthritis). If left unaddressed this condition worsens over time and can eventually require knee replacement surgery. To learn more about knee osteoarthritis check out our Guide to Knee Osteoarthritis.
Symptom: Knee pain when squatting, Knee pain when bending
- Knee pain when bending, kneeling, squatting, lunging, or any other position involving a deep knee bend can be the result of patellofemoral osteoarthritis, chondromalacia, or poor tracking of the patella (PFPS). Typically the further you push knee over your toes the more pain you will experience. A side-effect of this type of pain is significant muscle weakness. This can increase the severity of pain by creating a vicious cycle where one begins avoiding movements that would otherwise help strengthen your thigh muscles. Lifestyle modifications and a tailored exercise program can provide benefits here.
- Squatting without pain and with proper technique is a key marker of health. If you are having knee pain during squats and want to remedy it check out this blog: Knee Pain When Bending and Squatting
Symptom: Knee pain when running, Knee pain when exercising
- Knee pain when running, exercising or playing sports is the result of the high impact forces that can be many times your bodyweight. If the joint is not functioning optimally, this extra stress can lead to increased pain and dysfunction. Approximately 40% of running-related injuries are at the knee – the most common being6: (1) Patellofemoral Pain Syndrome, (2) Meniscal Injury, (3) Patellar Tendonitis and (4) Osteoarthritis. Technical factors such as foot strike and gait can affect how much pressure you put on your knees. If you want to learn more about what to do for knee pain while running, check out: Top Five Causes of Knee Pain while Running

Knee Injuries
Types of Knee Injury
Painful knee injuries can be divided into three categories:
- Traumatic: Significant damage to the knee such as ligament tears typically occur only when the knee is subjected to sudden unexpected forces. Pain and disability are immediate after these injuries, thus medical attention and diagnosis are often sought quickly afterward.
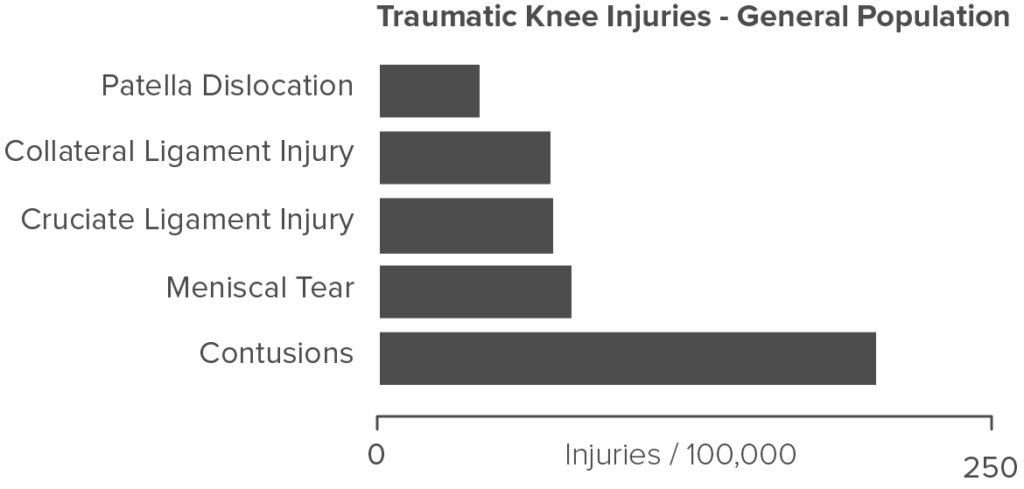

- Repetitive Strain: These types of injuries are typically associated with specific activities at work or while playing a sport. The same movement performed over and over again without adequate recovery puts the joint in a constant state of fragility and dysfunction. Patellar tendonitis and patellofemoral pain syndrome (PFPS) are the most common types of repetitive strain injuries of the knee.
- Degenerative Disorders: The common knee ailment in the world is osteoarthritis. A condition that tends to set in after the age of 50. Arthritis is the slow degradation of the surfaces and cushioning within one’s knee joint. Knee osteoarthritis is the most common cause of knee pain, affecting approximately 240 out of 100,000 individuals.7

- There are an estimated 14 million people in the USA suffering from symptomatic knee arthritis.
- There is a 45% chance you will develop symptomatic knee arthritis during your lifetime.8
Knee Osteoarthritis (OA)
The World Health Organization (WHO) reports that by 2050 over 130 million people will have osteoarthritis solidifying its position as the most common cause of knee pain. One-third of these individuals will be severely disabled.9 Osteoarthritis is the most common type of arthritis and the knee is the most common joint affected by the disease.
Most of us will show signs of osteoarthritis in our lifetime but not everyone experiences debilitating symptoms. However, if you are over the age of 50, and have recently developed consistent knee pain, there is a high probability you have osteoarthritis. Without intervention, this disease will slowly devour the cartilage in your knee leaving your joint in a painful bone on bone state. At this point, many opt for invasive knee replacement surgery. If you have osteoarthritis or you feel like it may be the underlying cause of your knee pain, check out our Guide to Severe Knee Arthritis for more information.
Meniscus Injury
As described earlier, your meniscus is a disc of cartilage cushioning that sits between your the end of your thigh bone and the top of your shin bone. When functioning normally it provides load transmission and shock absorption as you load up your knee joint.
Unfortunately tearing your meniscus means that you may suffer from osteoarthritis later in life. Ten to twenty years after the injury, 50% of those who had suffered a meniscus injury will have osteoarthritis.10 There is not much you can about this once you are injured. Prevention and preservation are the best options. Wearing a knee brace in a protective capacity, ensuring that you maintain muscle strength, and keeping your weight under control are all great options to ensure your knee stays as healthy as possible over the long term.
Knee Injury by Occupation
Some jobs are much more physically demanding than others requiring more walking, bending, squatting and kneeling. Over a lifetime the extra joint stress associated with these jobs could put you at higher risk for knee pain. The graph below shows the prevalence of arthritis relative to occupation.25 As you would expect workers in trades, skilled labor and farming tend to have the highest risk for arthritis. Generally, jobs that require frequent kneeling squatting accelerate the risk for knee osteoarthritis.26
. Occupation and knee pain: a community study. Osteoarthritis and Cartilage, 8(2), 78-81.")
Knee Injury by Sport
Not all sports and physical activities carry the same risk for knee pain and injury. Check the graph below for an overview of the activities that commonly cause knee pain.12
. Epidemiology of knee injuries among US high school athletes, 2005/06–2010/11. Medicine and science in sports and exercise, 45(3), 462.")

Whether you have suffered a sudden traumatic knee injury or your knee has simply been unusually stiff and sore for several weeks – Getting it checked by a healthcare professional is always a good move.
Doctor: Unless your injury requires emergency medical care the first stop is typically your doctor. While they are not specialized in treating knee ailments they have access to your medical history and can decide if a referral is necessary. They are also educated in a very broad array of treatment options.
Physical Therapist: If your injury requires exercise-based rehabilitation, bracing, or further diagnosis, physical therapists can provide tremendous value.
Diagnostic Imaging: If you experienced a traumatic injury such as an ACL or Meniscus tear, an X-ray or MRI is often required to assess the full extent of the damage.
Rheumatologist, Orthopaedic Surgeon, and Sports Medicine Doctor: For some knee injuries physiotherapy and over the counter pain medication are not enough. In these cases, a specialist can provide insight into more advanced solutions for knee pain. This could include surgical options or more advanced pharmaceutical treatments like cortisone shots.

Age
As you get older, your risk of degenerative disorders such as osteoarthritis increases. Approximately 50% of adults over the age of 65 have radiographic evidence of knee osteoarthritis.13 That being said there are some knee conditions affecting adolescents at a much higher rate than adults. Osgood schlatters disease predominantly affects children between 9-16 years of age – resulting in painful inflammation around the patellar tendon.14
Sex
Your sex has a major influence on your risk for a knee injury.
- Female basketball players are x3.5 more likely to rupture their ACL.15
- Women age 50-79 experienced cartilage degeneration in their knees at rates greater than 3 times that of men.16
- Women are 2.2 times as likely to develop Patellofemoral Pain Syndrome.17
Body Mass
- Individuals with unusually high BMI (≥25) are 3 times as likely to experience accelerated cartilage degeneration.18
- Having a BMI greater than 30 doubles your risk of knee pain across your lifespan.19
- Online BMI Calculator
Previous Injury
One of the largest risk factors for knee pain is having had knee pain or an injury in the past. A big reason for this is that injuries often result in a loss of function and muscle weakness. If not rehabilitated properly a lack strength in the thigh and calf muscles can increase your risk of traumatic injury. It is also well known that injuries to the ACL and Meniscus increase the risk for arthritis later in life.20
Joint Alignment
Varus Malalignment or “bowed legs” results in increased stress on the lateral structures of the knee such as Lateral Collateral Ligament and Lateral Tibiofemoral Joint Compartment.21 For these individuals, arthritis pain is more likely to be located on the outside of the knee.
Valgus Malalignment or “knock knees” is much more common than varus and is primarily caused by poor lower body strength and movement mechanics. As knees cave in under load, the MCL, ACL, Medial Meniscus, and Medial Tibiofemoral Joint Compartment are all under increased strain.
Patellar Tracking is a common cause of knee pain, particularly in active individuals. Typically, the lateral quadriceps muscles become stronger than those on the inside of the thigh (vastus medialis oblique) causing the kneecap to move too far laterally during knee extension. This creates abnormal friction and knee pain.22
Genetics
Your DNA is what makes you unique, and that also applies to your joints. Variation in the genes providing the blueprints for your connective tissue affects your joints resiliency and susceptibility to injury. If your parents had severe osteoarthritis you have up to a 25% increased risk of experiencing knee pain throughout life.23
Sport
Sports that involve frequent sprinting, running, jumping and cutting place the knee joint under tremendous loads. Football, soccer, basketball, and volleyball all have a high incidence of traumatic knee injuries and overuse knee injuries from training.
Training Load
Exercise and sport are worthwhile and healthy endeavors, however, too much of a good thing can increase the risk for injury. Field and court athletes who have a dense game schedule or are training heavily should be wary as their muscles may not provide the stability they typically do when fresh.25 Overuse injuries by definition occur when you place the same type of stress on the knees, in the same way, too often. These injuries typically occur during repetitive occupational tasks and sports with frequent jumping and running.
Muscular Strength
Muscle weakness is both the result of and a predictor of a knee injury.
- Your thigh muscles are essentially shock absorbers for the knee joint. Making sure that you have strong quadriceps and hamstrings is crucial for avoiding knee pain.
- Your glutes (gluteus medius, gluteus maximus) both help to stabilize your knee joint. Weakness in these muscles often results in the knees collapsing inwards (valgus stress)

Knee Pain Treatment
R.I.C.E
If you are suffering from an arthritis flare-up, or a mild strain, the treatments summarized in the acronym R-I-C-E are often prescribed by medical professionals.
 REST: Knee pain and inflammation are often a sign that there is some structural damage to your knee. If it’s mild in nature it often resolves within a week or two of rest. Resuming normal activities to soon could cause further structural damage and increase the required recovery time.
REST: Knee pain and inflammation are often a sign that there is some structural damage to your knee. If it’s mild in nature it often resolves within a week or two of rest. Resuming normal activities to soon could cause further structural damage and increase the required recovery time.
ICE: Once the knee joint is irritated, inflammation builds causing pain and stiffness. Exposing the affected area to cold temperatures constricts blood vessels and reduces the swelling.
COMPRESSION: The circulatory system requires muscle contraction to re-circulate blood back to your heart. When in pain, the tendency is to move the affected area less which causes fluid and inflammation to build up. Using a compression garment can help facilitate drainage and normal circulation.
ELEVATION: Just like compression elevating the injured leg above the heart can help reduce swelling and improve circulation.
Painkilling Drugs
 Over the Counter (OTC): Over the counter drugs like ibuprofen and acetaminophen can provide rapid relief from mild to moderate knee pain. These drugs are usually safe for short to medium-term use but require medical supervision for long periods of time.
Over the Counter (OTC): Over the counter drugs like ibuprofen and acetaminophen can provide rapid relief from mild to moderate knee pain. These drugs are usually safe for short to medium-term use but require medical supervision for long periods of time.
Prescription: Those suffering from severe pain are often candidates for more powerful NSAIDs like celecoxib or opioids. Typically these are prescribed after a traumatic injury, for people with severe arthritis, or post-surgically.
Exercise
 Exercise is the number one recommended treatment for knee pain. However, the type of exercise you should be doing really depends on the type of knee injury that you have. Generally exercise programs aimed at reducing knee pain attempt to strengthen the glutes, thighs, and calves. In order to ensure that you are performing the right exercise regime in the correct manner, consider consulting a physical therapist or personal trainer. Note that If your knee has suffered serious structural damage (Ruptured ACL, Torn Meniscus, etc.) exercise could be unsafe and may further damage your joints.
Exercise is the number one recommended treatment for knee pain. However, the type of exercise you should be doing really depends on the type of knee injury that you have. Generally exercise programs aimed at reducing knee pain attempt to strengthen the glutes, thighs, and calves. In order to ensure that you are performing the right exercise regime in the correct manner, consider consulting a physical therapist or personal trainer. Note that If your knee has suffered serious structural damage (Ruptured ACL, Torn Meniscus, etc.) exercise could be unsafe and may further damage your joints.
Bracing
Knee braces can be a great option for those experiencing instability and weakness in conjunction with their knee pain. There are a variety of different classes of knee brace that apply to different injuries.
 Knee Sleeves are usually made of elastic cotton or neoprene. The compression and warmth the garment provides can help decrease inflammation and keep your knee from feeling stiff.
Knee Sleeves are usually made of elastic cotton or neoprene. The compression and warmth the garment provides can help decrease inflammation and keep your knee from feeling stiff.
Stability Knee Braces can be soft or have a rigid frame the latter providing more support. This type of brace helps stop your knee from collapsing laterally (sideways) as you bend the joint.
Offloader Knee Braces are designed to address osteoarthritis specifically. These braces take pressure away from certain parts of the knee which helps reduce pain and preserve the integrity of the joint. Learn more – Top Five Offloader Knee Braces.
Rehabilitation Knee Braces are used after surgery to restrict the movement of the joint, ensuring proper healing of the joint. For example, ACL braces will often limit the degree to which you can straighten your knee.
Arthritis Solutions
If you or your doctor think arthritis is playing a role in your knee discomfort – learning more about the underlying cause of the condition can help you manage it now and in the future.
Glossary
Osteoarthritis: A degenerative disease that causes the cartilage to slowly disappear resulting in pain, stiffness, and a lack of joint mobility
Ligament: Tough fibrous ropes that connect bones together – structurally supporting joints.
Cartilage: Spongy tissue that sitting between bones providing load transmission and cushioning
Tendon: Elastics that connect muscle to bone allowing for energy transfer.
Bursa: A fluid-filled sack that sits near joints and muscles reducing friction during movement.
Get Rid of your Knee Arthritis Pain – Book Your Free Consultation Here
or give us a call at 1.877.209.8780
References
- Nguyen, U. S. D., Zhang, Y., Zhu, Y., Niu, J., Zhang, B., & Felson, D. T. (2011). Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. Annals of internal medicine, 155(11), 725-732.
- Bunt, C. W., Jonas, C. E., & Chang, J. G. (2018). Knee Pain in Adults and Adolescents: The Initial Evaluation. American family physician, 98(9).
- D’Lima, D. D., Fregly, B. J., Patil, S., Steklov, N., & Colwell Jr, C. W. (2012). Knee joint forces: prediction, measurement, and significance. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, 226(2), 95-102.
- Woolf, C. J. (2010). What is this thing called pain?. The Journal of clinical investigation, 120(11), 3742-3744.
- Schiphof, D., Van Middelkoop, M., De Klerk, B. M., Oei, E. H. G., Hofman, A., Koes, B. W., ... & Bierma-Zeinstra, S. M. A. (2014). Crepitus is a first indication of patellofemoral osteoarthritis (and not of tibiofemoral osteoarthritis). Osteoarthritis and cartilage, 22(5), 631-638.
- Taunton, J. E., Ryan, M. B., Clement, D. B., McKenzie, D. C., Lloyd-Smith, D. R., & Zumbo, B. D. (2002). A retrospective case-control analysis of 2002 running injuries. British journal of sports medicine, 36(2), 95-101.
- Oliveria, S. A., Felson, D. T., Reed, J. I., Cirillo, P. A., & Walker, A. M. (1995). Incidence of symptomatic hand, hip, and knee osteoarthritis among patients in a health maintenance organization. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology, 38(8), 1134-1141.
- Murphy LB, et al. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Rheum. 2008 Sep 15;59(9):1207-13.
- United Nations. World Population to 2300.
- Lohmander, L. S., Englund, P. M., Dahl, L. L., & Roos, E. M. (2007). The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. The American journal of sports medicine, 35(10), 1756-1769.
- O'Reilly, S. C., Muir, K. R., & Doherty, M. (2000). Occupation and knee pain: a community study. Osteoarthritis and Cartilage, 8(2), 78-81.
- Swenson, D. M., Collins, C. L., Best, T. M., Flanigan, D. C., Fields, S. K., & Comstock, R. D. (2013). Epidemiology of knee injuries among US high school athletes, 2005/06–2010/11. Medicine and science in sports and exercise, 45(3), 462.
- Anderson, A. S., & Loeser, R. F. (2010). Why is osteoarthritis an age-related disease?. Best practice & research Clinical rheumatology, 24(1), 15-26.
- Yashar A, Loder RT, Hensinger RN (1995). "Determination of skeletal age in children with Osgood-Schlatter disease by using radiographs of the knee". J Pediatr Orthop. 15 (3): 298–301.
- Ireland, M. L. (2002). The female ACL: why is it more prone to injury?. Orthopedic Clinics, 33(4), 637-651.
- Hanna, F. S., Teichtahl, A. J., Wluka, A. E., Wang, Y., Urquhart, D. M., English, D. R., ... & Cicuttini, F. M. (2009). Women have increased rates of cartilage loss and progression of cartilage defects at the knee than men: a gender study of adults without clinical knee osteoarthritis. Menopause, 16(4), 666-670.
- Boling, M., Padua, D., Marshall, S., Guskiewicz, K., Pyne, S., & Beutler, A. (2010). Gender differences in the incidence and prevalence of patellofemoral pain syndrome. Scandinavian journal of medicine & science in sports, 20(5), 725-730.
- Keng, A., Sayre, E. C., Guermazi, A., Nicolaou, S., Esdaile, J. M., Thorne, A., ... & Cibere, J. (2017). Association of body mass index with knee cartilage damage in an asymptomatic population-based study. BMC musculoskeletal disorders, 18(1), 517.
- Macfarlane, G. J., de Silva, V., & Jones, G. T. (2011). The relationship between body mass index across the life course and knee pain in adulthood: results from the 1958 birth cohort study. Rheumatology, 50(12), 2251-2256.
- Barenius, B., Ponzer, S., Shalabi, A., Bujak, R., Norlén, L., & Eriksson, K. (2014). Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up study of a randomized controlled trial. The American journal of sports medicine, 42(5), 1049-1057.
- Hinckel, B. B., Demange, M. K., Gobbi, R. G., Ricardo, J., & Camanho, G. L. (2016). The effect of mechanical varus on anterior cruciate ligament and lateral collateral ligament stress: finite element analyses. Orthopedics, 39(4), e729-e736.
- Dixit, Sameer, et al. "Management of patellofemoral pain syndrome." Am Fam Physician75.2 (2007): 194-20
- Pan, F., Ding, C., Winzenberg, T., Khan, H., Martel-Pelletier, J., Pelletier, J. P., ... & Jones, G. (2016). The offspring of people with a total knee replacement for severe primary knee osteoarthritis have a higher risk of worsening knee pain over 8 years. Annals of the rheumatic diseases, 75(2), 368-373.
- McMaster, C. (2013). Fatigue impact on non-contact ACL injury risk associated with multi-directional jumping and landing in female athletes: A systematic review. Journal of Science and Medicine in Sport, 16, e4–e5. doi:10.1016/j.jsams.2013.10.013
- Rossignol, M., Leclerc, A., Hilliquin, P., Allaert, F. A., Rozenberg, S., Valat, J. P., ... & Fautrel, B. (2003). Primary osteoarthritis and occupations: a national cross sectional survey of 10 412 symptomatic patients. Occupational and environmental medicine, 60(11), 882-886
- Palmer, K. T. (2012). Occupational activities and osteoarthritis of the knee. British medical bulletin, 102(1), 147-170.