What Is Patellofemoral Arthritis?

There are many types of arthritis. The most common type of arthritis is osteoarthritis. This disease can occur in multiple parts of your knee, such as the kneecap and one or both sides of your knee. One of the most prevalent forms of osteoarthritis occurs in your kneecap, which is a part of your patellofemoral compartment. This form of osteoarthritis is called patellofemoral arthritis.
Since arthritis is such a broad term, this article will first go over the differences between the most common types of arthritis, including osteoarthritis, rheumatoid, and gout. We will then dive further into the details of osteoarthritis, with a particular focus on patellofemoral arthritis.
What Is Arthritis?
There are over 100 diseases classified as arthritis1. To understand what these diseases have in common, all you need to do is break down the word “arthritis.” “Arthro-” is a prefix meaning “joint” while “-itis” means inflammation. So simply put, arthritis occurs when your joints begin to swell. This swelling leads to pain and loss of function at the affected joint.
It is important to understand that arthritis is a broad term that describes a collection of diseases. Even though these diseases affect your body in similar ways, they occur within your body for different reasons. As a result, they will require different treatment approaches.
Types of Arthritis: Many Different Faces
Even though many diseases are classified as “arthritis,” do not be fooled – they have many distinct differences. To help you get a sense of its range, below is a summary table showing the differences in six out of 100+ types of arthritis.
What you’ll notice is that arthritis can occur for many different reasons. And depending on what kind you have, it can also have different risk factors, treatment options, and health consequences.
Six Major Forms of Arthritis Compared
| Type of Arthritis | Overview |
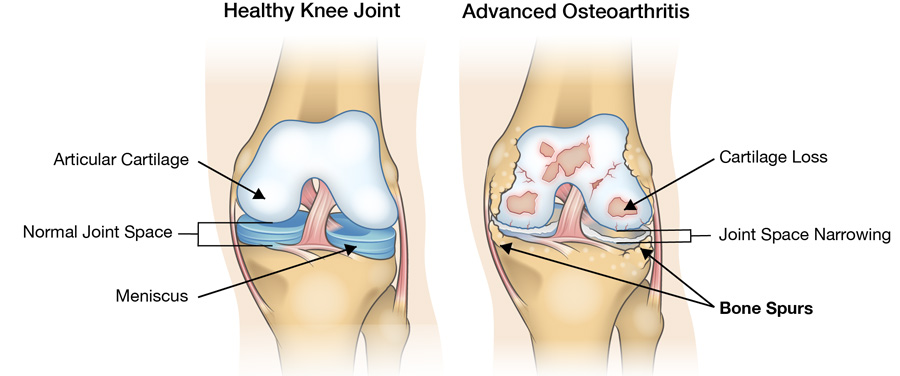
| Osteoarthritis | Degradation of your articular cartilage, which is the smooth surface covering your bones. In your knee, this cartilage reduces friction within your patellofemoral and tibiofemoral compartments. Without this protective layer, your bones will rub together, causing inflammation and pain. |
| Rheumatoid Arthritis | A type of autoimmune disease, rheumatoid arthritis occurs when your immune system mistakenly attacks itself. Since autoimmune diseases are systemic (affecting the whole body), rheumatoid not only causes inflammation in your joints, but can also affect your skin, eyes, lungs, and heart. |
| Gout | A build-up of urate crystals within your joint, which results in inflammation. Uric acid is a normal byproduct created within your body and is usually disposed of through your kidneys. If you have too much uric acid, or your kidneys cannot keep up with disposal, it can crystallize within your body causing inflammation in your joints. |
| Reactive Arthritis | Joint inflammation caused by an infection in your body. |
| Psoriatic Arthritis | May occur if you already suffer from psoriasis, a disorder resulting in red, thick, itchy skin. However, joint inflammation and pain may occur before you are diagnosed with a skin condition. |
| Ankylosing Spondylitis | Inflammation in your spine, which may eventually cause the bones in your spine to grow and attach, limiting mobility. |
What Is Patellofemoral Arthritis?
In Canada, osteoarthritis affects more people than all the other types of arthritis combined. For the rest of this article, we will focus on osteoarthritis, and more specifically, osteoarthritis of the patellofemoral joint. To keep things simple, we will refer to osteoarthritis of the patellofemoral joint as patellofemoral arthritis.
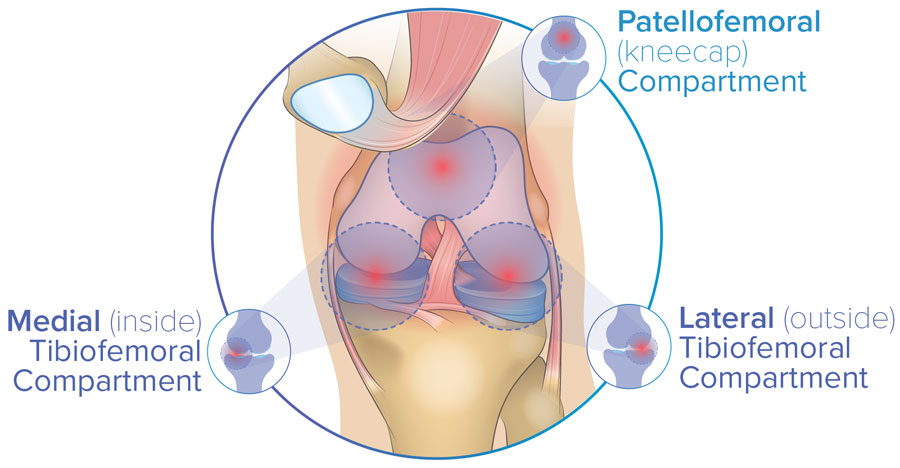
The patellofemoral compartment is a point of contact between two of your bones. The knee joint is made up of three bones: your femur, tibia, and patella. Two of these points of contact are between your femur and tibia (the medial and lateral tibiofemoral compartments). The third compartment is between your femur and patella (patellofemoral compartment).
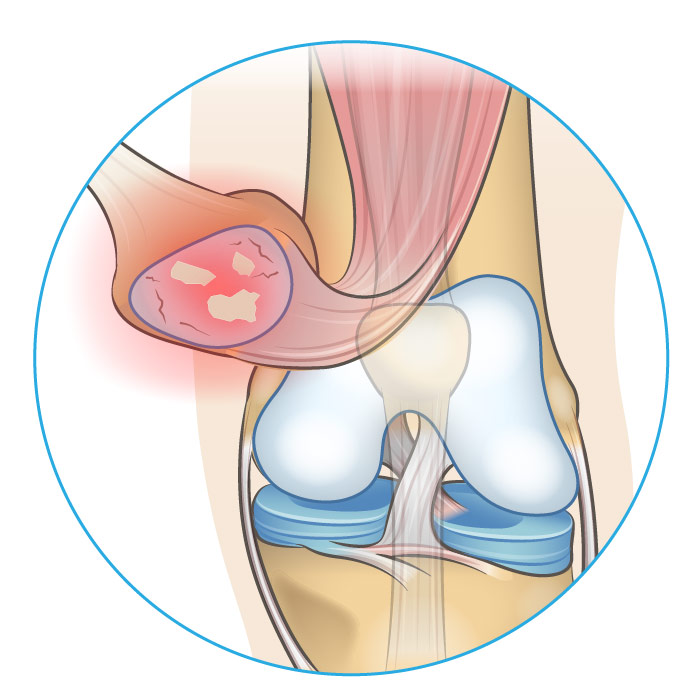
We already know that osteoarthritis occurs because your articular cartilage degrades, causing higher friction between your bones. In the case of patellofemoral arthritis, too much friction is between your patella and femur. This friction will cause pain in the patellofemoral compartment when you bend your knee, like when you rise from sitting, go up and down the stairs, or squat.
Patellofemoral Arthritis: More Common Than You Think
Osteoarthritis is the most common joint disorder in the United States2. It has been recorded that one in seven adults in the United States suffer from osteoarthritis3. That translates to 32.5 million people living with the condition. A similar burden can be seen in Canada, with 1 in 8 (3.9 million people) over the age of 20 living with osteoarthritis4.
Osteoarthritis is also prevalent globally. Worldwide, approximately four out of five osteoarthritis cases involve the knee5. And recent study involving almost 4000 knees with osteoarthritis found that 63% of conditions involved the patellofemoral compartment6.
These statistics are alarming. It is also alarming that these numbers are only rising. Results from a recent study indicated that knee osteoarthritis has doubled in prevalence since the mid-20th century7. To explain, lifespans and BMI (body mass index) are predicted to keep on rising, which will increase the prevalence of osteoarthritis8.
Finally, on top of having patellofemoral arthritis, you can have arthritis in your other knee compartments. In fact, it is quite common to have osteoarthritis in two or even all three compartments of the knee.
Why Did I Get Patellofemoral Arthritis?
Osteoarthritis is a complex disease. In fact, it is so complex that professionals in the field cannot predict who will develop the disease. The Osteoarthritis Research Society International has been working since 1990 to answer some fundamental questions that will help predict the onset of osteoarthritis. Even though we do not have all the answers, there are some known facts about risk factors for patellofemoral arthritis:
- Age: Patellofemoral articular cartilage degeneration can result from general wear and tear9. As you age, so does your body. As your knees get old, they naturally become worn down.
- Gender: Past the age of 65, women are more than twice as likely to develop patellofemoral osteoarthritis than men10. There are a couple of reasons why this may occur. For example, women tend to gain weight faster than men after they experience menopause. Additionally, women have wider hips than men, which can cause different pressure distributions within the knee compartments.
- Weight: You are more likely to develop osteoarthritis if you are overweight11 [11]. The more weight you carry on your body, the higher the forces are that pass through your knee compartments. This can accelerate the wear and tear of your articular cartilage.
- Past injury: The development of osteoarthritis can be accelerated if you have had a previous knee injury12. This could result from a knee dislocation or fracture, cartilage damage, meniscus tear, or tendon injury. You may be at higher risk of developing patellofemoral arthritis if you have patellar misalignment13. If the patella does not move correctly within the groove of the femur, it may undergo higher than normal pressures in certain locations. These elevated pressures may speed up further degeneration of articular cartilage.
How Do I Manage Patellofemoral Arthritis?
Arthritis is considered a chronic disease, which means there is no cure that will make it disappear forever. Luckily, there are many options available to help you manage the symptoms. The pain and mobility restrictions caused by arthritis can prevent you from doing what you love to do. To help you get moving again, the following sections explore possible options.
Weight Loss and Exercise
The amount of pressure going through your joints is directly related to your body weight. If you are able to reduce your weight and remain physically active, you may be able to slow down the rate at which your patellofemoral osteoarthritis progresses14.
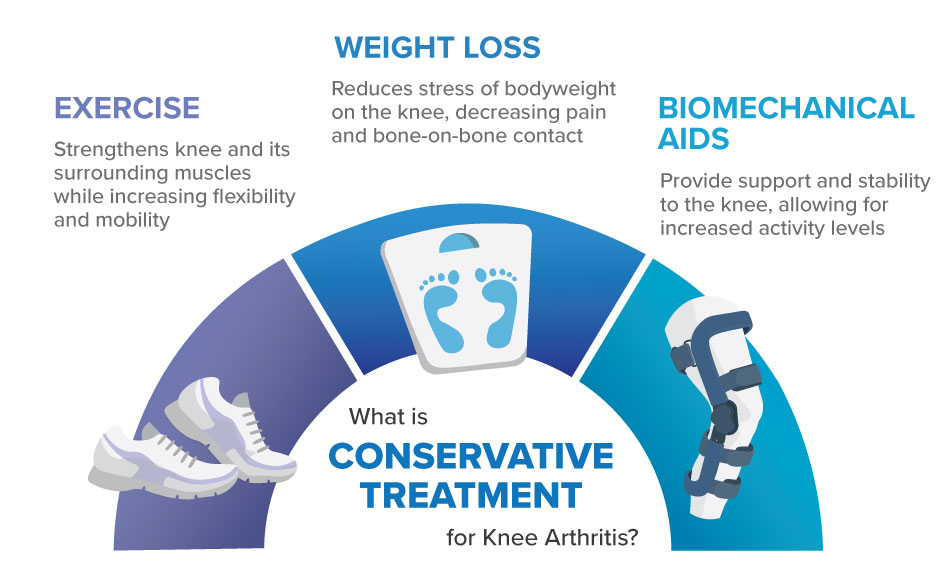
Exercises that help you improve mobility and gain quadriceps (upper leg) strength may help you manage your symptoms. This is because having stronger quadriceps can help stabilize your patella and delay the progression of patellofemoral arthritis.
If you are already suffering from pain related to patellofemoral arthritis, the idea of doing physical activity may be daunting. Using an assistive device, such as a knee brace, may help you manage an exercise routine. We recommend reaching out to a health care professional and using reliable resources that can help you navigate what type of activities are best for your knee.
Exercise, weight loss, and biomechanical devices are all forms of conservative treatment. If you want to learn more about treatments that do not involve painkillers or surgery, take a look at our Guide to Conservative Treatment.
Knee Bracing

Braces can help improve your mobility, reduce your pain, and protect your knee joint. It can be difficult to navigate among the many knee braces on the market. However, when it comes to managing your symptoms of patellofemoral arthritis, you have one primary goal. This goal is the reduction of pressure within your patellofemoral joint. Simply put, you need a brace that will absorb a portion of your body weight so your knee experiences less wear and tear.
The only brace that is appropriate for patellofemoral knee pain is a tri-compartment offloader (TCO). The Levitation knee brace is the world’s first and only TCO knee brace. Proven to provide clinically relevant knee offloading in all three knee compartments of the knee21,22, this brace is appropriate for all patterns of knee osteoarthritis.
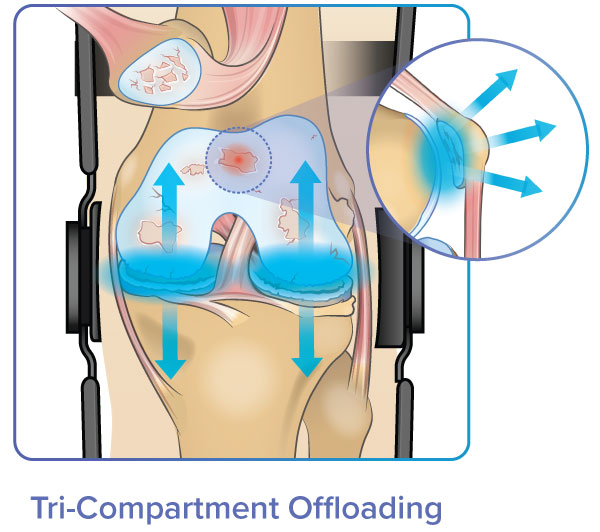
How does tri-compartment offloading work? Levitation stores energy within a patented mechanical spring and returns this energy in the form of knee extension assistance. As a result, users experience total pressure relief across the entire knee.
Additionally, Levitation’s extension assistance helps you straighten (extend) your leg, therefore reducing the amount of force going through all three compartments of your knee. This brace also promotes strengthening of the quadriceps muscles, allowing you to rebuild your strength while you regain your mobility.
Want to learn if Levitation is right for you? Click the button below to schedule a consultation with a bracing specialist. Consultations are completely free and done virtually or over the phone.
Medications and Injections
Medications such as acetaminophen (Tylenol) and nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen can be useful for treating the symptoms of patellofemoral arthritis [15]. Topical NSAIDs options are available and recommended as they promote local therapy, compared to oral NSAIDs which provide systematic (full body) exposure [15].

Steroid injections such as cortisone are powerful anti-inflammatories that can temporarily help you manage your symptoms. Viscosupplement injections contain a thick fluid called hyaluronic acid, which can help lubricate your knee joint and reduce friction between bones [16].
Other types of injections used for osteoarthritis include stem cell injections and PRP shots.
However, all these medications and injections are temporary and have their associated side effects. Always talk to your health care professional before taking oral or topical medications or injections for your patellofemoral arthritis symptoms.
Surgery
Generally, surgery should be the last option when it comes to knee osteoarthritis. Depending on your age and the severity of your condition, one of the below surgical interventions may be an option for you.
Minimally Invasive or Preventative Surgeries
- Arthroscopic Chondroplasty: Damaged cartilage is trimmed and removed through a small incision in your knee, allowing new tissue to grow. This procedure is minimally invasive and has a shorter recovery period compared to other knee surgeries. However, chondroplasty is not often the most appropriate intervention unless your arthritis is mild and you experience symptoms of knee catching or locking17.
- Partial Lateral Patellar Facetectomy: Removal of 1-1.5 cm of bone from the lateral (outside) area of the patella (kneecap). This procedure is appropriate for reducing symptoms for individuals with patellofemoral osteoarthritis who also have bone spurs caused by excessive friction18.
- Tibial Tuberosity Osteotomy: A procedure that improves the alignment of the patella relative to the femur. This procedure changes the location at which the patellar tendon meets the tibia. By improving patella tracking, the procedure can help redistribute the forces between your patella and femur and delay the early onset of osteoarthritis19.
Knee Replacement Surgeries
- Patellofemoral Knee Replacement: This is a partial knee replacement where the patella and a section of the femur are resurfaced with a metal or plastic implant to reduce friction between the bones. This intervention may be optimal if both sides of your knee (medial and lateral tibiofemoral compartments) are arthritis-free20.
- Total Knee Replacement (TKR): More common than partial replacement, TKR can help manage symptoms in all three compartments of the knee. According to the American Academy of Orthopedic Surgeons, TKR should be the last resort due to high procedural costs, its invasive nature, the risk of complications, and the need for revision surgery.
Thinking about total knee replacement? Check out our related resources to learn more:
- Video of Knee Replacement Surgery
- How Long Do Knee Replacements Last? The Truth
- An In-Depth Look at Knee Replacement Recovery Time
References
- “Frequently Asked Questions (FAQs) about Arthritis | CDC,” Feb. 21, 2019. https://www.cdc.gov/arthritis/basics/faqs.htm (accessed Jun. 03, 2021).
- Y. Zhang and J. M. Jordan, “Epidemiology of Osteoarthritis,” Clinics in Geriatric Medicine, vol. 26, no. 3, pp. 355–369, Aug. 2010, doi: 10.1016/j.cger.2010.03.001.
- “Osteoarthritis | BMUS: The Burden of Musculoskeletal Diseases in the United States.” https://www.boneandjointburden.org/fourth-edition/iiib10/osteoarthritis (accessed Jun. 03, 2021).
- P. H. A. of Canada, “Osteoarthritis in Canada,” Sep. 29, 2020. https://www.canada.ca/en/public-health/services/publications/diseases-conditions/osteoarthritis.html (accessed Jun. 03, 2021).
- T. Vos et al., “Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013,” The Lancet, vol. 386, no. 9995, pp. 743–800, Aug. 2015, doi: 10.1016/S0140-6736(15)60692-4.
- J. C. Stoddart, O. Dandridge, A. Garner, J. Cobb, and R. J. van Arkel, “The compartmental distribution of knee osteoarthritis – a systematic review and meta-analysis,” Osteoarthritis and Cartilage, vol. 29, no. 4, pp. 445–455, Apr. 2021, doi: 10.1016/j.joca.2020.10.011.
- I. J. Wallace et al., “Knee osteoarthritis has doubled in prevalence since the mid-20th century,” Proc Natl Acad Sci USA, vol. 114, no. 35, pp. 9332–9336, Aug. 2017, doi: 10.1073/pnas.1703856114.
- A. Turkiewicz et al., “Current and future impact of osteoarthritis on health care: a population-based study with projections to year 2032,” Osteoarthritis and Cartilage, vol. 22, no. 11, pp. 1826–1832, Nov. 2014, doi: 10.1016/j.joca.2014.07.015.
- D. R. Carter, G. S. Beaupré, M. Wong, R. L. Smith, T. P. Andriacchi, and D. J. Schurman, “The Mechanobiology of Articular Cartilage Development and Degeneration,” Clinical Orthopaedics & Related Research, vol. 427, pp. S69–S77, Oct. 2004, doi: 10.1097/01.blo.0000144970.05107.7e.
- “Osteoarthritis Risk Factors in Women & How to Prevent Them,” Hospital for Special Surgery. https://www.hss.edu/conditions_why-women-higher-risk-getting-arthritis.asp (accessed Jun. 03, 2021).
- Z.-Y. Zhou, Y.-K. Liu, H.-L. Chen, and F. Liu, “Body mass index and knee osteoarthritis risk: A dose-response meta-analysis: Body Mass Index and Knee Osteoarthritis Risk,” Obesity, vol. 22, no. 10, pp. 2180–2185, Oct. 2014, doi: 10.1002/oby.20835.
- A. M. Bhosale and J. B. Richardson, “Articular cartilage: structure, injuries and review of management,” British Medical Bulletin, vol. 87, no. 1, pp. 77–95, Aug. 2008, doi: 10.1093/bmb/ldn025.
- S. R. Ward, M. R. Terk, and C. M. Powers, “Patella Alta: Association with Patellofemoral Alignment and Changes in Contact Area During Weight-Bearing,” The Journal of Bone & Joint Surgery, vol. 89, no. 8, pp. 1749–1755, Aug. 2007, doi: 10.2106/JBJS.F.00508.
- G. D. Deyle, N. E. Henderson, R. L. Matekel, M. G. Ryder, M. B. Garber, and S. C. Allison, “Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of the Knee: A Randomized, Controlled Trial,” Ann Intern Med, vol. 132, no. 3, p. 173, Feb. 2000, doi: 10.7326/0003-4819-132-3-200002010-00002.
- S. L. Kolasinski et al., “2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee,” Arthritis Rheumatol, vol. 72, no. 2, pp. 220–233, Feb. 2020, doi: 10.1002/art.41142.
- “Viscosupplementation Treatment for Arthritis.” https://www.hopkinsmedicine.org/health/conditions-and-diseases/arthritis/viscosupplementation-treatment-for-arthritis (accessed Jun. 03, 2021).
- J. B. Moseley et al., “A Controlled Trial of Arthroscopic Surgery for Osteoarthritis of the Knee,” N Engl J Med, vol. 347, no. 2, pp. 81–88, Jul. 2002, doi: 10.1056/NEJMoa013259.
- L. E. Paulos, D. L. O’Connor, and A. Karistinos, “Partial Lateral Patellar Facetectomy for Treatment of Arthritis Due to Lateral Patellar Compression Syndrome,” Arthroscopy: The Journal of Arthroscopic & Related Surgery, vol. 24, no. 5, pp. 547–553, May 2008, doi: 10.1016/j.arthro.2007.12.004.
- N. L. Grimm, A. L. Lazarides, and A. Amendola, “Tibial Tubercle Osteotomies: a Review of a Treatment for Recurrent Patellar Instability,” Curr Rev Musculoskelet Med, vol. 11, no. 2, pp. 266–271, Jun. 2018, doi: 10.1007/s12178-018-9482-3.
- HSS, “Patellofemoral Arthritis of the Knee: An Overview,” Hospital for Special Surgery. https://www.hss.edu/conditions_patellofemoral-arthritis-in-the-knee-overview.asp (accessed Jun. 03, 2021).
- C. A. McGibbon, S. Brandon, E. L. Bishop, C. Cowper-Smith, and E. N. Biden, “Biomechanical Study of a Tricompartmental Offloader Brace for Patellofemoral or Multicompartment Knee Osteoarthritis,” Front. Bioeng. Biotechnol., vol. 8, 2021, doi: 10.3389/fbioe.2020.604860.
- A. R. Budarick, B. E. MacKeil, S. Fitzgerald, and C. D. Cowper-Smith, “Design Evaluation of a Novel Multicompartment Offloader Knee Brace,” J Biomech Eng, vol. 142, no. 1, Jan. 2020, doi: 10.1115/1.4044818.