Knee Pain on the Front of Your Joint? Learn Why.
If you are active and value mobility there is nothing worse than crippling knee pain. It worsens your quality of life and if not addressed properly it can become a recurring problem. Knee pain on the front of the joint (anterior knee pain) is a common complaint, particularly for those who are physically active. The first step to ridding yourself of this nagging issue is determining the underlying cause.
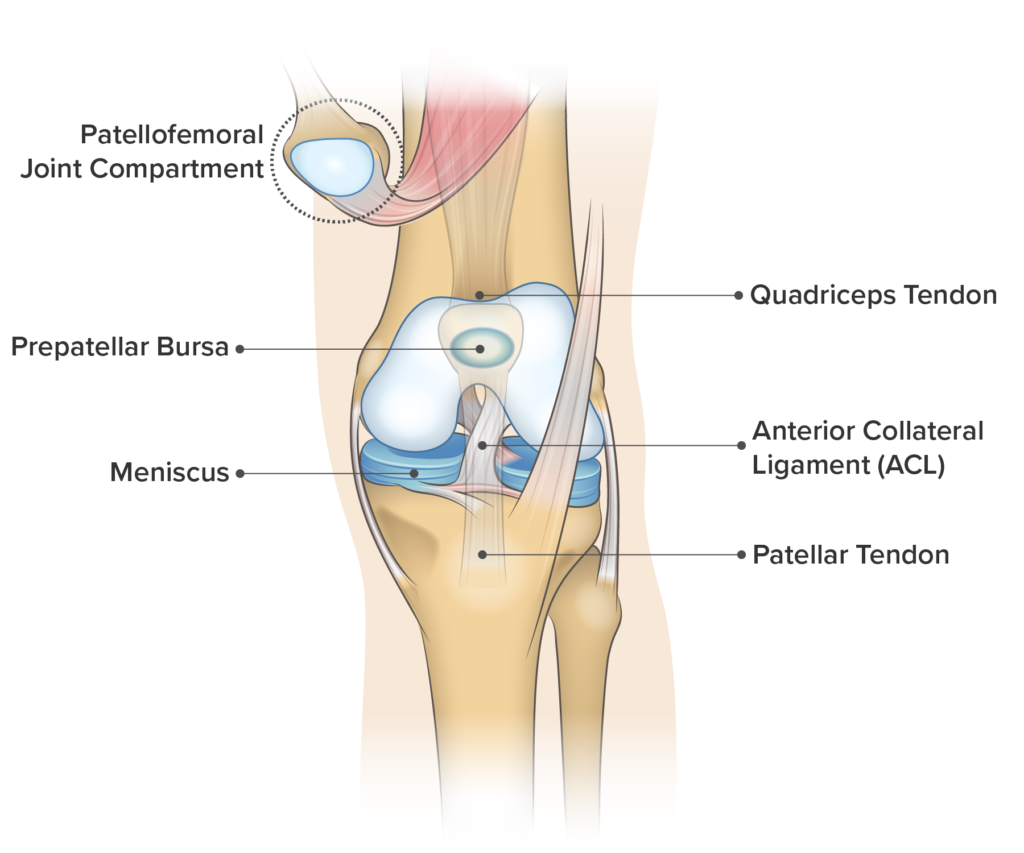
Knee Pain on the Front of Your Joint
Knee Tendonitis | Patellofemoral Pain Syndrome | Chondromalacia Patella | Knee Arthritis | ACL Strain/Sprain | Patellar Fracture | Pre-patellar Bursitis
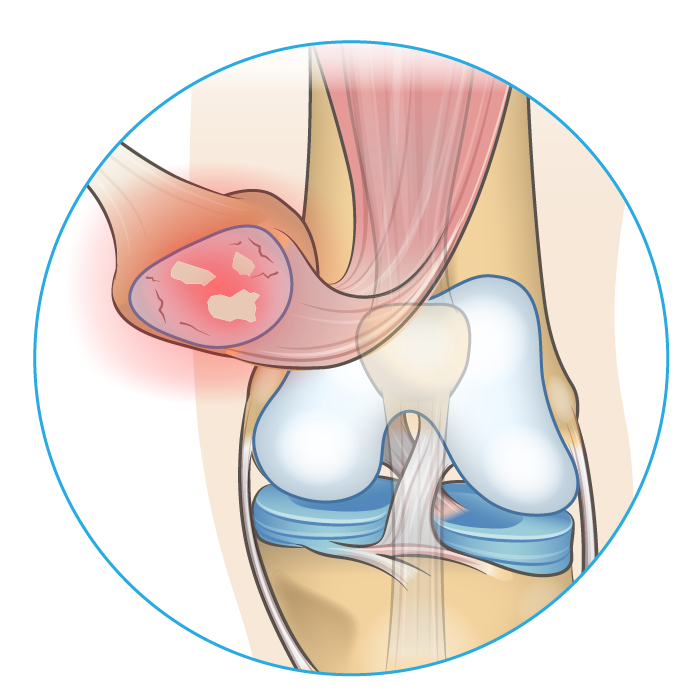
Knee Tendonitis
Cause & Symptoms
Tendonitis related knee pain typically occurs during and after periods of abnormally elevated physical activity. High-risk activities include running and jumping. Symptoms include tenderness to the touch and sharp localized pain on the front of your knee. While the root cause of tendonitis is still not fully understood, scientists believe it is the result of a failed healing response.1 This can be confirmed via diagnostic imaging using doppler ultrasound. Afflicted tendons display abnormal structural changes including increased thickness and a higher density of blood vessels (vascularity).4 There are three common subtypes of tendonitis that can affect your knees:
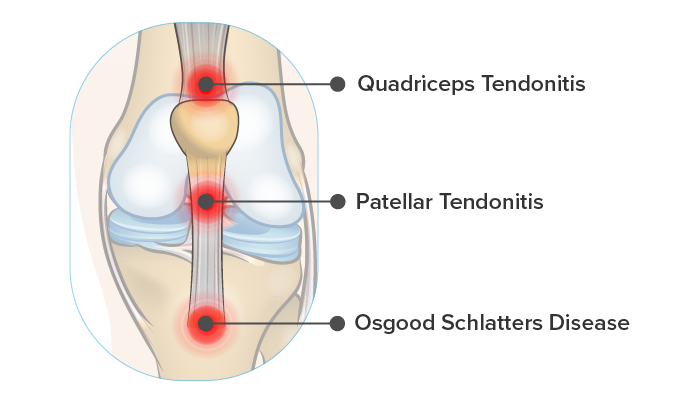
- Quadriceps Tendonitis
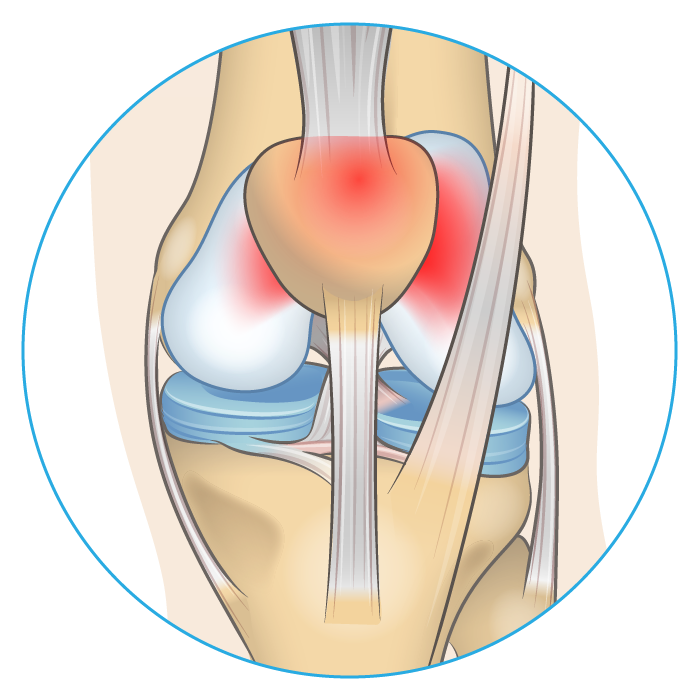
Quadriceps tendonitis makes up just 20% of knee tendonitis related cases.2 It is characterized by pain and tenderness at the top of the knee cap and often occurs alongside patellar tendonitis.4
- Patellar Tendonitis
The patellar tendon connects your knee cap to your shin bone. Injury to this tendon is very common in athletes that participate in jumping sports – 40% of volleyball players suffer from patellar tendonitis at some point in their career.3
- Osgood Schlatters & Patellar Insertional Tendonitis
Sometimes patellar tendonitis can be localized around the tendon’s insertion point at the top of the shin bone. Over time, the area can begin to calcify leaving a prominent bony bump. This is commonly seen in Osgood Schlatter’s disease, a condition that occurs in adolescents particularly after growth spurts. Osgood Schlatters presents identically to insertional patellar tendonitis but tends to resolve on its own over time.
Treatment
The gold standard for tendon rehabilitation is a combination of quadriceps stretching, resistance training and temporarily stopping activities that cause pain.1 Tendonitis can be thought of as a rough patch job that keeps your tendon structurally sound, with the tradeoff being stiffness and pain. A specific protocol administered by a physiotherapist can help promote tissue healing. Try to be patient – tendon tissue heals much more slowly than muscle tissue.
Patellofemoral Pain Syndrome (PFPS)
Cause & Symptoms
PFPS is one of the most common causes of knee pain accounting for 25-40% of knee pain related problems at sports injury clinics.5 Symptoms include grinding sensations when bending the knee joint, tenderness around the kneecap, swelling, and pain when rising from a sitting position.5 The cause of PFPS is unclear and likely complex. Abnormal joint alignment, quadriceps muscle weakness, and poor hip stability have all been identified as potential causes.5
Treatment
Quadriceps and hip strengthening are the most effective methods for eliminating pain associated with PFPS.6 Rehabilitation programs usually consist of a variety of exercises that challenge muscular strength and balance. A physiotherapist or personal trainer can supply you with exercise programming and instruction appropriate to your unique situation. If you are in need of immediate relief consider patellar taping. Here a physiotherapist will use special adhesive tape to help guide your kneecap to the proper position on the joint – reducing grinding and pain on the front of your joint.6
Chondromalacia Patella
Cause & Symptoms
Chondromalacia Patella is very similar to PFPS, and many consider them to be the same condition.7 You can think of it as advanced PFPS where abnormal joint friction has caused the cartilage on the underside of the kneecap to become damaged. The symptoms and causes remain largely the same other than genetic risk factors for poor cartilage repair making some individuals more prone to chondromalacia than others.7
Treatment
Treatment usually involves a combination of resistance exercise, stretching and activity modifications similar to that of PFPS. If the condition persists it could eventually lead to patellofemoral osteoarthritis.
Patellofemoral Osteoarthritis
Cause & Symptoms
Healthy joint movement is low friction joint movement. Over your lifetime the kneecap slides over the surface of the thigh bone (femur) countless times. Articular cartilage coating the underside of the knee cap allows for smooth pain-free movement when you bend your leg. For many of us, this cartilage will slowly wear away exposing bone on the underside of the patella to other bony surfaces within the joint. This is an early sign of knee osteoarthritis. As the disease progresses painful bone spurs develop leaving you stiff, inflamed, and experiencing significant pain on the front of the knee. Knee osteoarthritis disproportionately affects the elderly but can afflict people in their early twenties.8
Treatment
Unfortunately, there is no known cure for knee osteoarthritis. Most treatments focus on slowing down joint degeneration and controlling symptoms. In extreme cases where the disease is severely limiting the patient’s quality of life full knee replacement surgery is considered. To learn more about the vast array of treatment strategies available to you check out: Guide to Severe Knee Arthritis Treatment Options
Anterior Cruciate Ligament (ACL) Sprain/Strain
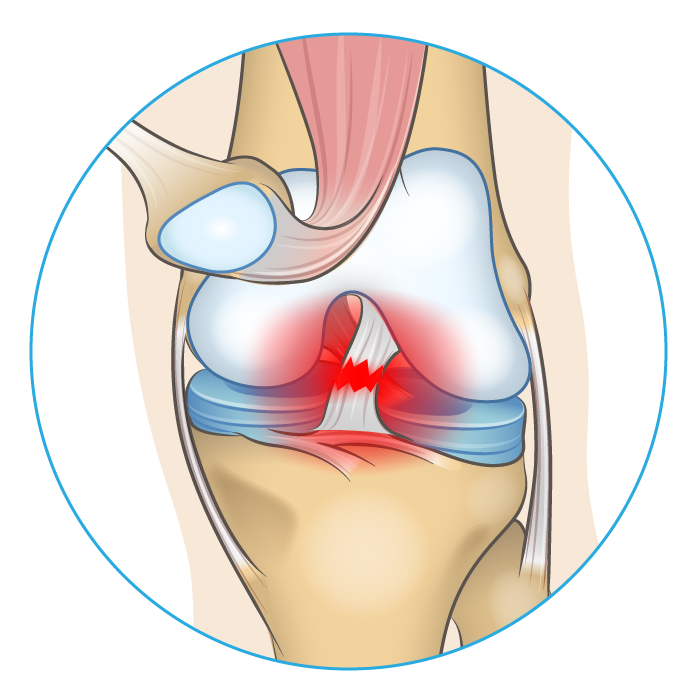
Cause & Symptoms
If you watch or play sports you are probably quite familiar with ACL injuries. These injuries typically occur during player on player contact (42%), or noncontact, occurring at high speeds where an athlete attempts to brake or change direction (38%).9 Women are almost twice as likely to experience an ACL injury. Pain and dysfunction localized at the front of the knee will begin immediately after the injury. Additionally, due to the nature of the injury, other knee structures such as the lateral and medial collateral ligaments often experience trauma as well.
- Grade I: The ACL has been overstretched, while there is no major damage, its function will be compromised until it has healed.
- Grade II: The ACL has been partially torn and may require surgery to repair depending on the extent of the damage.
- Grade III: A complete tear of the ACL requiring surgery to reconstruct the ligament.
Treatment
Over 70% of ACL injuries require surgery.9 One common issue after injury and the subsequent surgery is poor proprioception – your ability to sense the position of a joint in time and space. Ligaments are rich in receptors that enable proprioception. As a result, when you injure your ACL you will experience joint instability. Overcoming this requires months of commitment to strengthening and balancing exercises.
Patellar Fracture
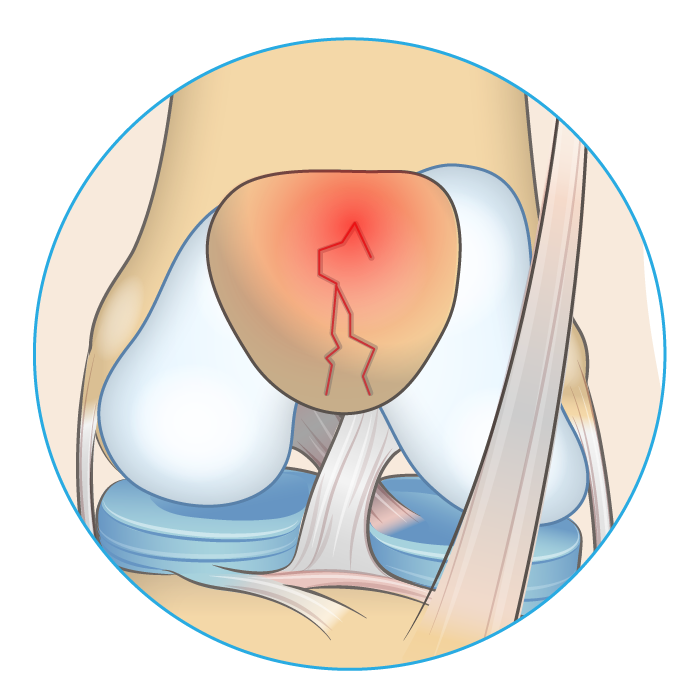
Cause & Symptoms
Blunt force trauma applied to the knee cap can cause a bone fracture leading to extreme pain on the front of the knee. In extreme cases, the kneecap may split either horizontally or vertically.
Treatment
Surgery is often required to resolve patellar fractures. Separated pieces of bone are sutured back together to reform the kneecap. Recovery is slow – weight bearing on the injured leg is typically prohibited for 6-8 weeks.10
Prepatellar Bursitis
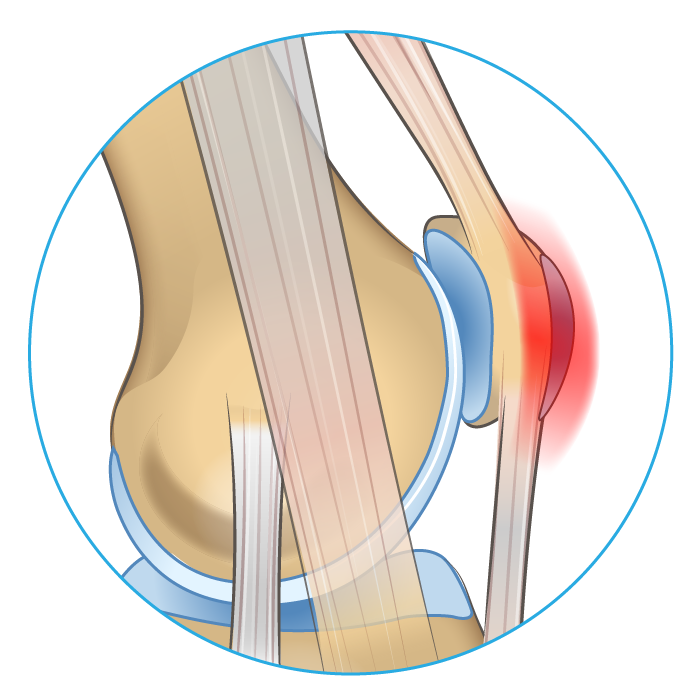
Cause & Symptoms
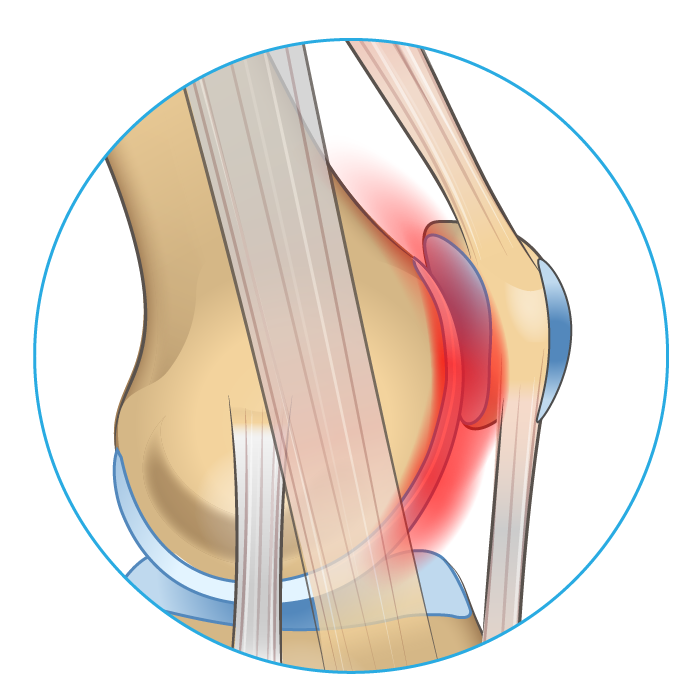
Bursae are small fluid-filled sacs that help reduce friction between sliding surfaces. The prepatellar bursa is located on the front of the knee cap. Bursitis is the overproduction of synovial fluid within the bursa. In prepatellar bursitis, this causes massive swelling and pain on the front of the knee. The cause is typically direct trauma to the knee cap or irritation from repetitive occupational movement. Over 80% of patients are male and are typically between 40-60 years of age.11
Treatment
Solutions vary depending on the severity of the fluid build-up. In mild cases, the RICE Method may be enough to resolve symptoms. If the bursa continues to swell or is unresponsive to conservative treatment, a needle can be inserted to drain excess fluid. Some more extreme situations such as infection may require the bursa to be surgically removed.11
What’s Next?
Hopefully, this information helped you narrow down the cause of your knee pain. We hope you find a speedy resolution to your condition or injury. In the meantime, if you want to learn more, check out the resources below.
References
- Peters, J. A., Zwerver, J., Diercks, R. L., Elferink-Gemser, M. T., & van den Akker-Scheek, I. (2016). Preventive interventions for tendinopathy: A systematic review. Journal of Science and Medicine in Sport, 19(3), 205–211. doi:10.1016/j.jsams.2015.03.008
- Ferretti, A. (2015). Patellar and Quadriceps Tendinopathy. Football Traumatology, 93–98.doi:10.1007/978-3-319-18245-2_10
- Ferretti A (1986) Epidemiology of jumper’s knee. Sports Med 3(4):289–295
- King, D., Yakubek, G., Chughtai, M., Khlopas, A., Saluan, P., Mont, M. A., & Genin, J. (2019). Quadriceps tendinopathy: a review—part 1: epidemiology and diagnosis. Annals of translational medicine, 7(4).
- Crossley, K. M., van Middelkoop, M., Callaghan, M. J., Collins, N. J., Rathleff, M. S., & Barton, C. J. (2016). 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 2: recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions). Br J Sports Med, 50(14), 844-852.
- Crossley, K. M., van Middelkoop, M., Callaghan, M. J., Collins, N. J., Rathleff, M. S., & Barton, C. J. (2016). 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions). Br J Sports Med, 50(14), 844-852.
- Salehi-Abari, I., Khazaeli, S., & Niksirat, A. (2015). Chondromalacia Patella and New Diagnostic Criteria. Open Science Journal of Clinical Medicine, 3(4), 126-8.
- Anderson, A. S., & Loeser, R. F. (2010). Why is osteoarthritis an age-related disease?. Best practice & research Clinical rheumatology, 24(1), 15-26.
- Joseph, A. M., Collins, C. L., Henke, N. M., Yard, E. E., Fields, S. K., & Comstock, R. D. (2013). A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. Journal of athletic training, 48(6), 810-817.
- https://orthoinfo.aaos.org/en/diseases–conditions/patellar-kneecap-fractures
- Bumbach, S. F., Lobo, C. M., Badyine, I., Mutschler, W., & Kanz, K. G. (2014). Prepatellar and olecranon bursitis: literature review and development of a treatment algorithm. Archives of orthopaedic and trauma surgery, 134(3), 359-370.